

Review
doi: 10.1055/s-0038-1673422.
Epub 2018 Nov 5.
Thermal Ablation of Bone Metastases
Affiliations
- PMID: 30402013
- PMCID: PMC6218262
- DOI: 10.1055/s-0038-1673422
Item in Clipboard
Review
Thermal Ablation of Bone Metastases
Semin Intervent Radiol.
2018 Oct.
Abstract
Image-guided, minimally invasive, percutaneous thermal ablation of bone metastases has unique advantages compared with surgery or radiation therapy. Thermal ablation of osseous metastases may result in significant pain palliation, prevention of skeletal-related events, and durable local tumor control. This article will describe current thermal ablation techniques utilized to treat bone metastases, summarize contemporary evidence supporting such thermal ablation treatments, and outline an approach to percutaneous ablative treatment.
Keywords: cancer pain; interventional radiology; osseous metastases; pain palliation; thermal ablation.
Figures

Imaging of the ablation zone. (
a
) On MRI, the ablation zone during cryoablation (CA) appears as an area of hypointensity (
black arrows
) on all sequences. (
b
) CA zone is readily visible with CT as a hypoattenuating region in the soft tissue surrounding bone or in an osteolytic defect as well as within the marrow cavity (
arrows
). Its margins are not evident in cortical or other dense bone. (
c
) The ablation zone during radiofrequency ablation is not visible on CT. Instead, only a few bubbles of gas (
arrow
) are seen within the treated tumor from vaporization of intralesional fluid.
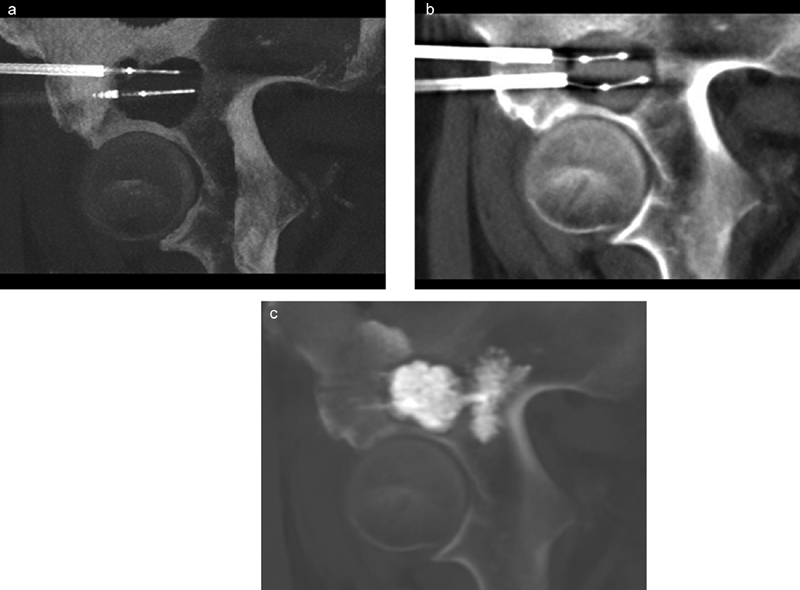
Palliative radiofrequency ablation (RFA) and cementoplasty of a painful right supra-acetabular renal cell carcinoma metastasis that progressed despite prior radiation therapy in a 64-year-old man. (
a
) Intraprocedural sagittal maximum intensity projection (MIP) image shows two bipolar RFA electrodes within the osteolytic metastasis. Note the electrodes were biased away from the hip joint during placement to avoid injury to the femoral head. (
b
) Using coaxial technique, the electrodes were replaced with vertebral augmentation balloons following ablation to create an adequate cavity for cement filling, given the tumor location in a weight-bearing bone. (
c
) Final sagittal MIP image shows excellent filling of the cavity, with cement tied into normal bone to create a solid construct.
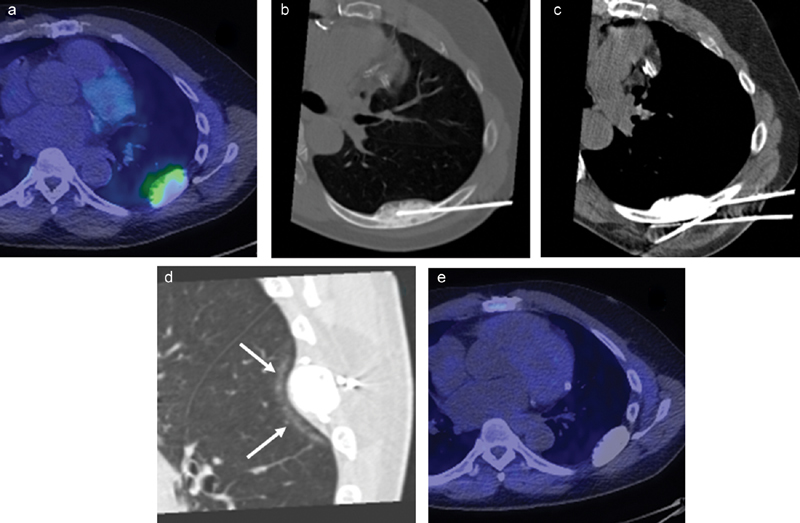
Cryoablation (CA) of oligometastatic disease from prostate carcinoma in a 52-year-old man with persistent PSA following prostatectomy and systemic therapy. (
a
) C11-choline PET/CT shows uptake within a sclerotic left 7th rib oligometastasis. CA was offered to obtain local tumor control. (
b
) Oblique axial CT image shows a cryoprobe advanced partially through the metastasis. Due to the tumor's dense sclerosis, a deeper tract could not be created with either a bone biopsy needle or handheld drill; so, the cryoprobe could not be placed deep enough to cover the posterior margin of the metastasis. (
c
) Instead, cryoprobes were placed along the margins of the rib to shape an ablation zone that would cover the entire tumor. As ice easily crosses through intact cortical and sclerotic bone, this strategy is acceptable even for a goal of local tumor control. (
d
) Intraprocedural sagittal CT image shows interstitial changes in the lung (
arrows
) deep to the metastasis along the edge of the ice ball, confirming adequate tumor coverage. (
e
) Follow-up PET/CT 1 year after ablation shows no uptake in the treated rib metastasis consistent with no residual tumor.

Combined cryoablation (CA) and radiofrequency ablation (RFA) followed by cementoplasty for pain palliation. (
a
) Intraprocedural CT image shows an osteolytic left periacetabular metastasis from renal cell carcinoma in a 65-year-old man with pain rated as 9/10 in severity, causing loss of sleep. (
b
) CA was performed on the superior aspect of the tumor, given relatively large size. (
c
) Bipolar RFA with an articulating electrode was used to treat the lower portion of the metastasis while avoiding the femoral head. (
d and e
) Cementoplasty was then performed to consolidate this metastasis at risk for pathologic fracture.
References
-
- Chow E, Zeng L, Salvo N, Dennis K, Tsao M, Lutz S. Update on the systematic review of palliative radiotherapy trials for bone metastases. Clin Oncol (R Coll Radiol) 2012;24(02):112–124. - PubMed
-
- Janjan N. Bone metastases: approaches to management. Semin Oncol. 2001;28(04) 11:28–34. - PubMed
-
- Saad F, Lipton A, Cook R, Chen Y M, Smith M, Coleman R. Pathologic fractures correlate with reduced survival in patients with malignant bone disease. Cancer. 2007;110(08):1860–1867. - PubMed
-
- Kurup A N, Callstrom M R. Ablation of musculoskeletal metastases: pain palliation, fracture risk reduction, and oligometastatic disease. Tech Vasc Interv Radiol. 2013;16(04):253–261. - PubMed
