

Review
doi: 10.1055/s-0038-1669963.
Epub 2018 Nov 5.
Endovascular Therapy for Lower Extremity Chronic Deep Venous Occlusive Disease: State of Practice
Affiliations
- PMID: 30402016
- PMCID: PMC6218266
- DOI: 10.1055/s-0038-1669963
Item in Clipboard
Review
Endovascular Therapy for Lower Extremity Chronic Deep Venous Occlusive Disease: State of Practice
Semin Intervent Radiol.
2018 Oct.
No abstract available
Figures
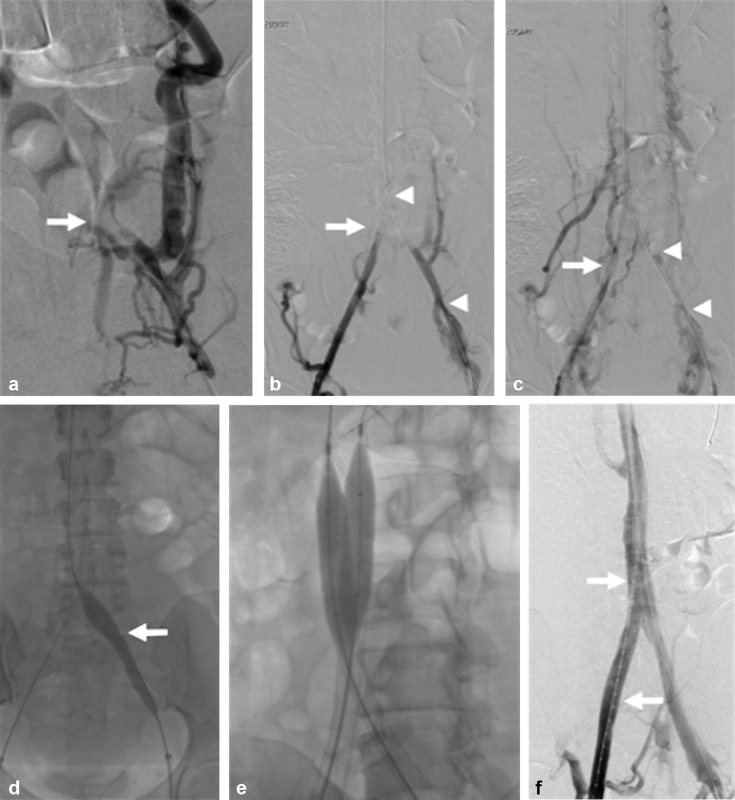
A 52-year-old female with quadriplegia, factor V Leiden, and antithrombin III deficiency referred for chronic iliocaval thrombosis and phlegmasia. (
a
) Left iliocaval venography demonstrating left common iliac occlusive disease with robust retroperitoneal collaterals. The iliocaval confluence is faintly seen (arrow). (
b
) Bilateral right (arrow) and left (arrowheads) iliocaval venography after blunt recanalization of the left iliac vein. (
c
) Bilateral right (arrow) and left (arrowheads) iliocaval venography after blunt recanalization of the right and left iliac veins. (
d
) Sequential angioplasty of the inferior vena cava was performed using 8 mm × 8 cm Mustang, 14 mm × 6 cm, and 18 mm × 4 cm Atlas balloons. Angioplasty of the bilateral right and left (arrow) common iliac veins was performed using 8 mm × 8 cm Mustang, 14 mm × 6 cm and 16 mm × 4 cm Atlas balloons. (
e
) Iliocaval reconstruction was performed using a 20 mm × 55 mm Wallstent within the inferior vena cava and 14 mm × 90 mm Wallstents within the bilateral common iliac veins. Postdeployment angioplasty was performed. (
f
) Completion venography showing brisk flow throughout the iliocaval venous reconstruction. A flush catheter is seen throughout the right iliocaval segments (arrows).
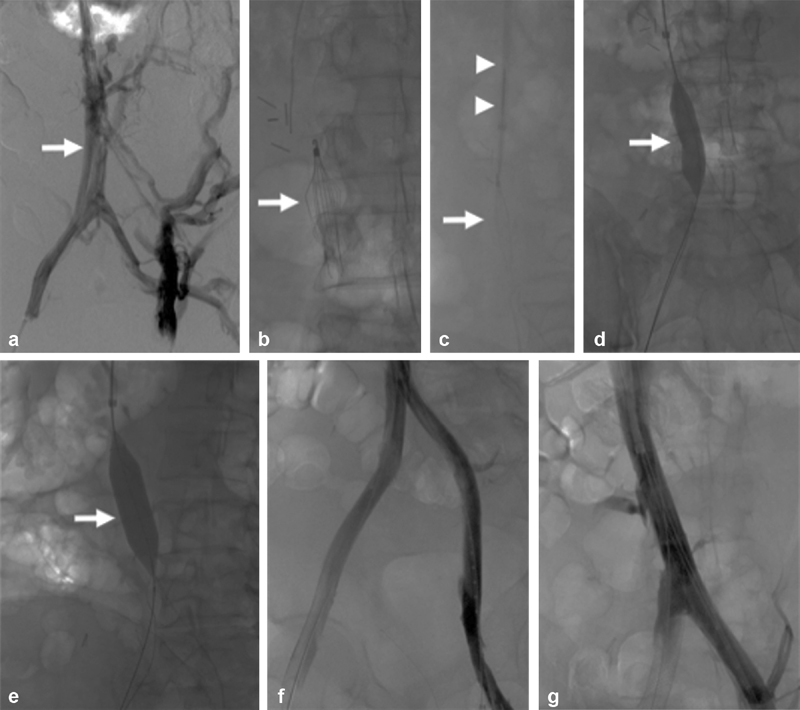
A 46-year-old male with esophageal cancer–associated hypercoagulability and inferior vena cava filter–associated chronic iliocaval thrombosis and left lower extremity ulceration (Clinical, Etiology, Anatomy, and Pathophysiology class 6 disease). (
a
) Bilateral iliocaval venography demonstrates chronic thrombotic changes throughout the iliac vein and inferior vena cava (arrow). Multiple lumbar and retroperitoneal venous collaterals are seen. (
b
) Fluoroscopic image showing a Denali inferior vena cava filter (arrow) causing chronic filter-associated iliocaval thrombosis. (
c
) The Denali inferior vena cava filter (arrow) was removed using the standard Cook retrieval set (arrowheads). (
d
) Angioplasty of the inferior vena cava using a 14-mm high-pressure balloon (arrow). (
e
) Angioplasty of the inferior vena cava using an 18-mm high-pressure balloon (arrow). (
f
) A 20 mm × 55 mm Wallstent was deployed in the inferior vena cava and 14 mm × 60 mm Wallstents were placed within the common iliac veins. Completion venography demonstrated robust in-line venous flow throughout both iliac veins. (
g
) Venography demonstrated in-line flow throughout the inferior vena cava.
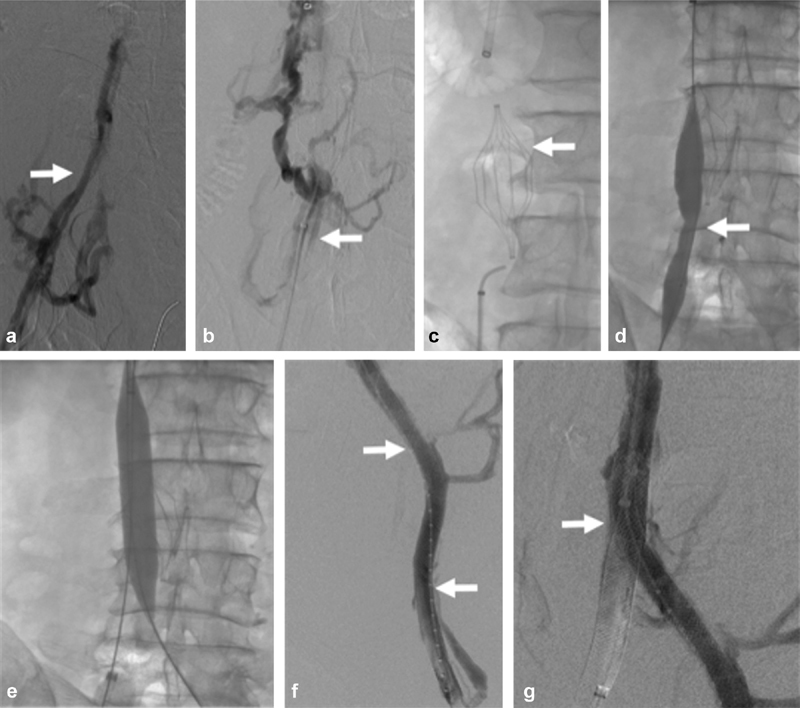
A 61-year-old male with methylenetetrahydrofolate reductase and smoking history with inferior vena cava filter–associated chronic iliocaval thrombosis and left lower extremity pain and swelling (Clinical, Etiology, Anatomy, and Pathophysiology class 4 disease). (
a
) Right iliocaval venography demonstrated venous irregularity consistent with chronic iliocaval thrombosis of the right iliocaval segment (arrow). (
b
) Initial attempts to cross the inferior vena cava filter–associated iliocaval thrombosis using a glidewire and glide catheter (arrow) were unsuccessful. (
c
) Fluoroscopic image demonstrating the Trapeze inferior vena cava filter (arrow) causing chronic filter-associated iliocaval thrombosis. Sharp recanalization was performed using a BRK needle and a loop snare. (
d
) Attempts to remove the inferior vena cava filter were unsuccessful. Angioplasty across the inferior vena cava filter was performed using a 4-mm Sterling balloon (arrow). (
e
) The infrarenal inferior vena cava was angioplastied using an 18-mm balloon) (
f
) A 20 mm × 55 mm Wallstent was deployed in the inferior vena cava and 12 mm × 90 mm Wallstents were deployed in the common iliac veins (arrows). (
g
) Completion venography demonstrated a briskly filling iliocaval reconstruction with Trapeze inferior vena cava filter sequestration (arrow).
Similar articles
-
"Modern Endovascular Therapy".World J Surg. 2021 Dec;45(12):3493-3502. doi: 10.1007/s00268-020-05875-7. Epub 2020 Nov 22. World J Surg. 2021. PMID: 33225390 Review.
-
Endovascular Interventions for Acute and Chronic Lower Extremity Deep Venous Disease: State of the Art.Radiology. 2015 Jul;276(1):31-53. doi: 10.1148/radiol.2015132603. Radiology. 2015. PMID: 26101920 Free PMC article. Review.
-
Endovascular management of venous thrombotic and occlusive diseases of the lower extremities.J Vasc Interv Radiol. 2003 Apr;14(4):405-23. doi: 10.1097/01.rvi.0000064849.87207.4f. J Vasc Interv Radiol. 2003. PMID: 12682198 Review.
-
Open surgical repair versus endovascular therapy for chronic lower-extremity occlusive disease.Annu Rev Med. 2003;54:269-83. doi: 10.1146/annurev.med.54.101601.152509. Epub 2001 Dec 3. Annu Rev Med. 2003. PMID: 12414919 Review.
-
A systematic review of venous stents for iliac and venacaval occlusive disease.J Vasc Surg Venous Lymphat Disord. 2020 Jan;8(1):145-153. doi: 10.1016/j.jvsv.2019.08.015. Epub 2019 Nov 5. J Vasc Surg Venous Lymphat Disord. 2020. PMID: 31699668
Cited by
-
Novel mechanical thrombectomy device used to restore patency to chronically occluded deep venous bypasses.J Vasc Surg Cases Innov Tech. 2025 May 24;11(4):101862. doi: 10.1016/j.jvscit.2025.101862. eCollection 2025 Aug. J Vasc Surg Cases Innov Tech. 2025. PMID: 40641516 Free PMC article.
-
Hybrid CT-angiography to facilitate lower extremity sharp venous recanalization: a novel approach to a common procedure.CVIR Endovasc. 2020 Oct 8;3(1):51. doi: 10.1186/s42155-020-00145-y. CVIR Endovasc. 2020. PMID: 33030614 Free PMC article.
References
-
- Raju S. Treatment of iliac-caval outflow obstruction. Semin Vasc Surg. 2015;28(01):47–53. - PubMed
-
- Williams D M. Iliocaval reconstruction in chronic deep vein thrombosis. Tech Vasc Interv Radiol. 2014;17(02):109–113. - PubMed
-
- Neglén P, Raju S. Balloon dilation and stenting of chronic iliac vein obstruction: technical aspects and early clinical outcome. J Endovasc Ther. 2000;7(02):79–91. - PubMed
-
- Neglén P, Darcey R, Olivier J, Raju S. Bilateral stenting at the iliocaval confluence. J Vasc Surg. 2010;51(06):1457–1466. - PubMed
