

Review
doi: 10.1055/s-0038-1673362.
Epub 2018 Nov 5.
Global Approach to the Patient with Pain in Interventional Radiology
Affiliations
- PMID: 30402017
- PMCID: PMC6218264
- DOI: 10.1055/s-0038-1673362
Item in Clipboard
Review
Global Approach to the Patient with Pain in Interventional Radiology
Semin Intervent Radiol.
2018 Oct.
No abstract available
Figures
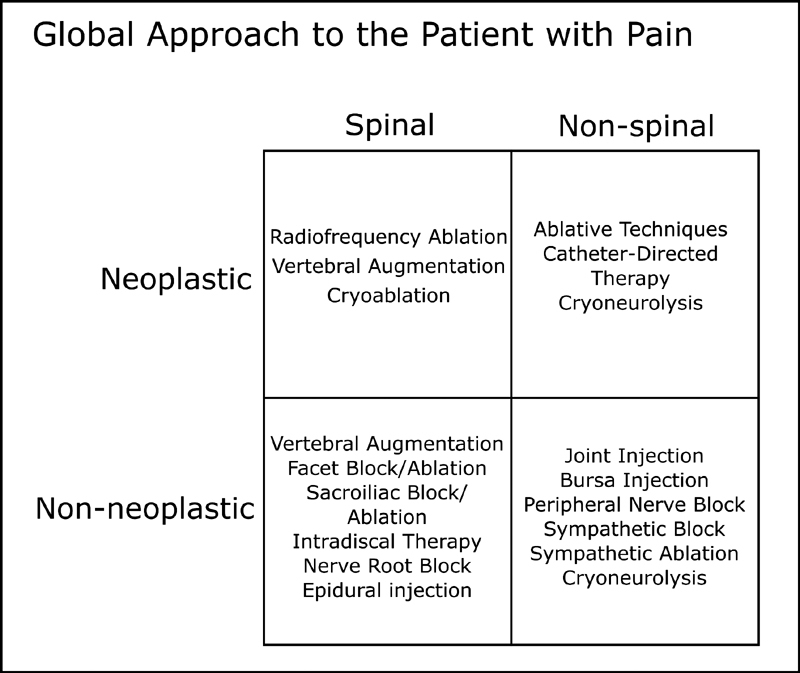
Global approach to the patient with pain.
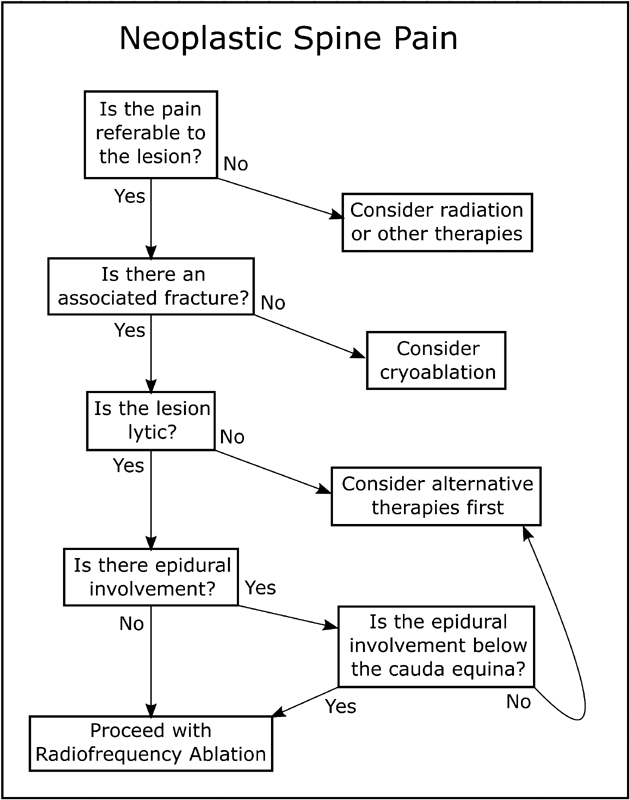
Algorithm for the evaluation of a painful metastatic lesion involving the spine.
(
a
,
b
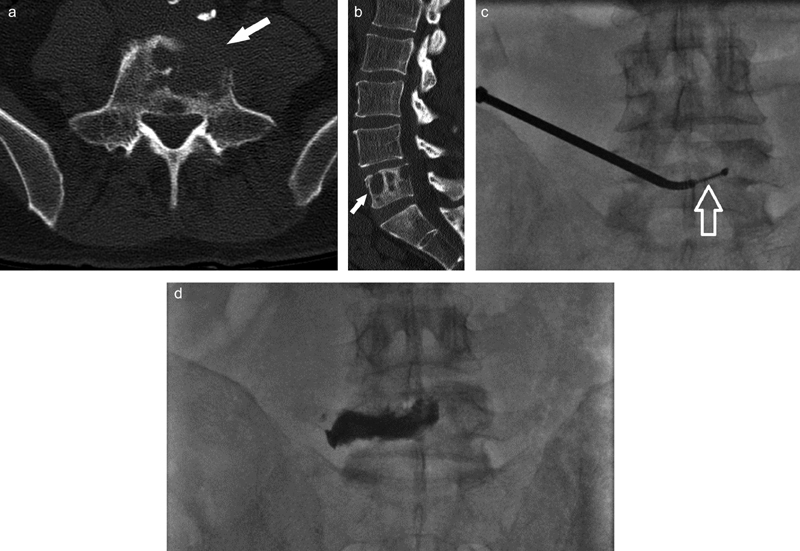
) Axial and sagittal CT images of a 57-year-old man with a history of lung cancer presenting with lumbar spine pain demonstrating lytic metastases involving L5 (
arrows
). (
c
) Intraprocedural anteroposterior (AP) image demonstrates a unipediculate coaxial, transpedicular approach from the left with a coaxially placed radiofrequency ablation probe (
arrow
) in the affected vertebral body. (
d
) Final image from RFA and cementoplasty demonstrates distribution of cement corresponding to the original lesion and fracture, providing stabilization.
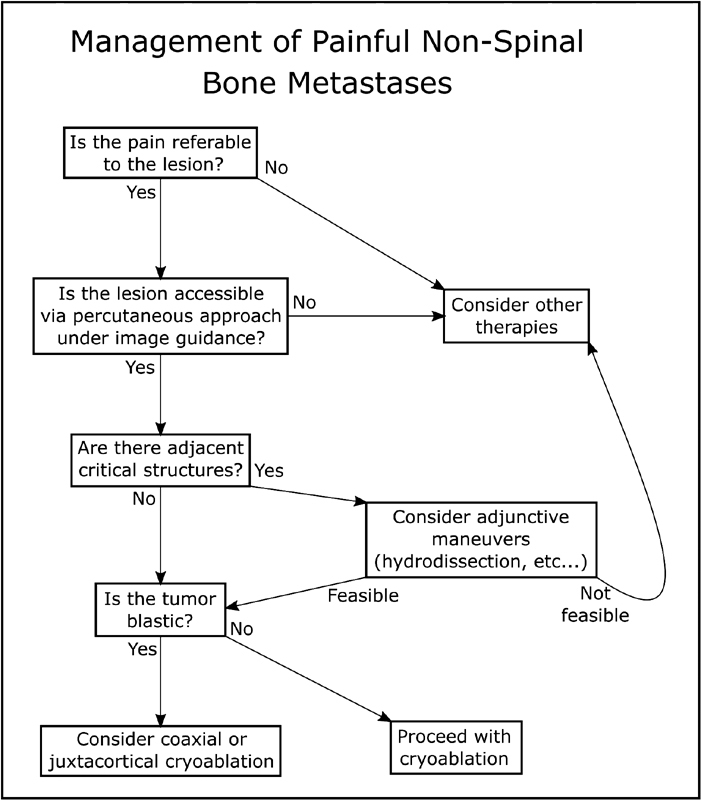
Algorithm for the evaluation of a painful metastatic lesion outside of the spine.
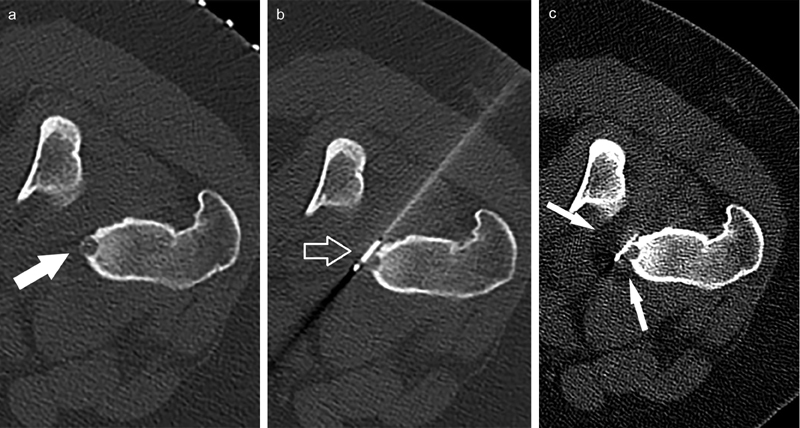
Axial intraprocedural CT images demonstrate a proximal femoral osteoid osteoma (
arrow
) in a 29-year-old man (
a
), subsequent juxtacortical percutaneous image-guided placement of a 17-gauge cryoablation probe (
b
,
arrow
), and demonstration of target lesion inclusion by the visualized ablation zone (
c
,
arrows
).
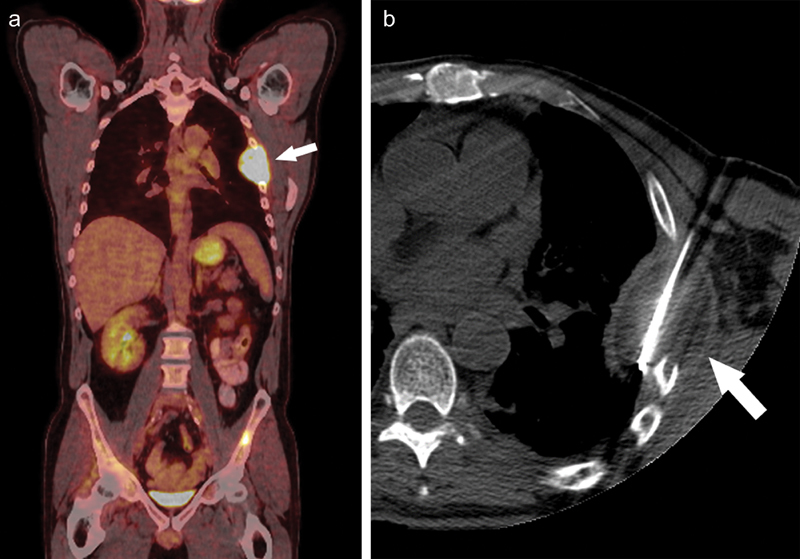
(
a
) A coronal fused image of a 71-year-old man with a history of non-small cell lung cancer and left chest wall pain demonstrates abnormal uptake of radiopharmaceutical about a left lateral rib (
arrow
), corresponding with his chief complaint. (
b
) Single axial intraprocedural CT image demonstrates placement of a 17-gauge cryoablation probe to the center of the lesion and the associated early ablation zone (
arrow
). In cases such as these, additional cryoablation probes or extension of freeze times are warranted to include the entirety of the lesion.
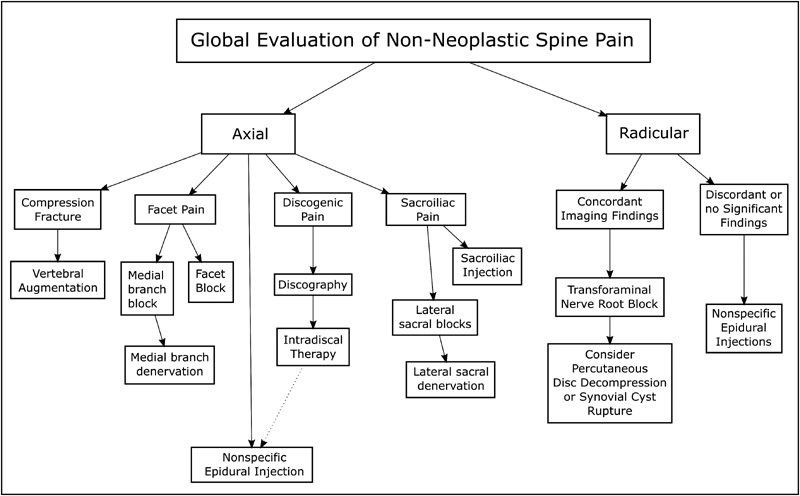
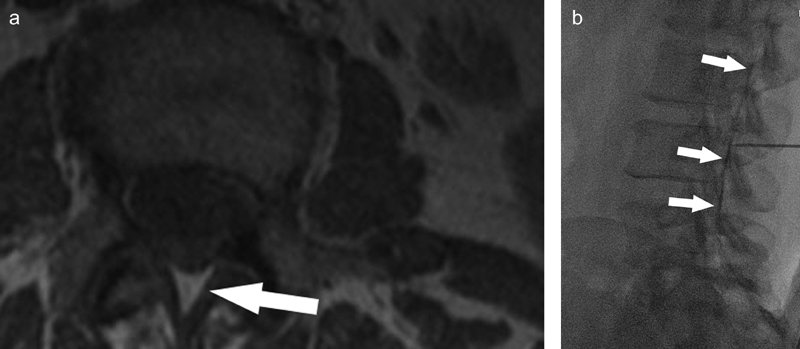
An algorithm for the management of nonneoplastic spine pain.
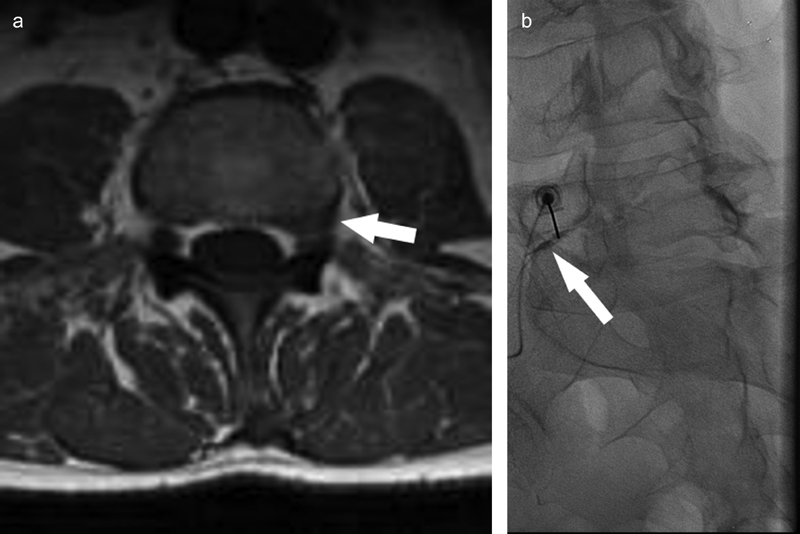
(
a
) Single axial T2-weighted MRI image demonstrates a left-side L5 asymmetric partial intervertebral disc herniation (
arrow
), corresponding to the patients presenting complaint. (
b
) Corresponding intraprocedural fluoroscopic image from a left-side L5 transforaminal injection demonstrates contrast outlining the affected exiting nerve root (
arrow
), confirming appropriate needle position.
(
a
) Single axial T1-weighted MRI image of the lumbar spine demonstrates the shape and location of the midline epidural space (
arrow
). (
b
) Corresponding intraprocedural fluoroscopic image demonstrates contrast outlining the midline epidural space (
arrows
), confirming appropriate needle position.
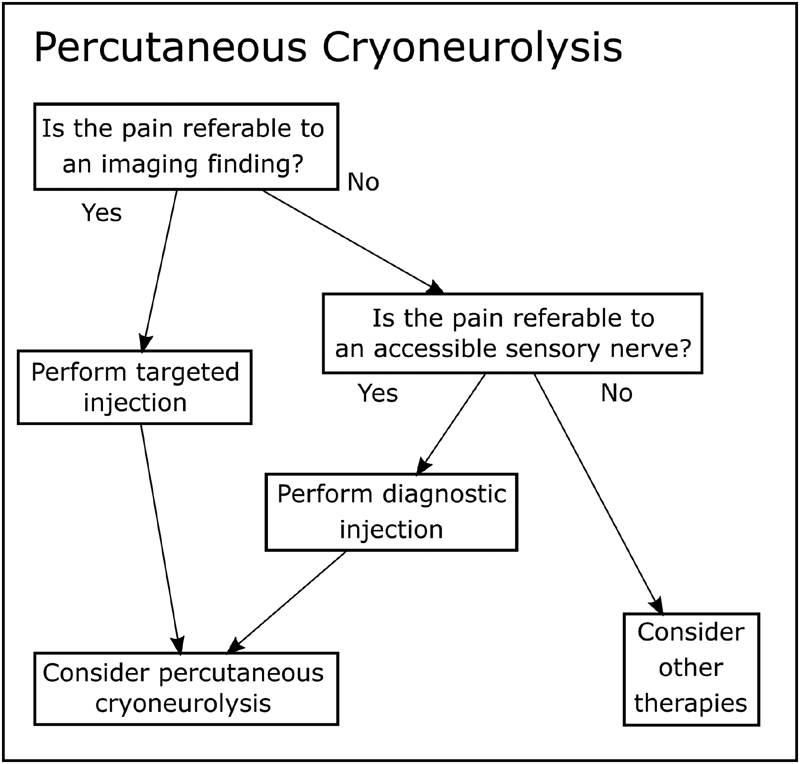
Percutaneous cryoneurolysis algorithm.
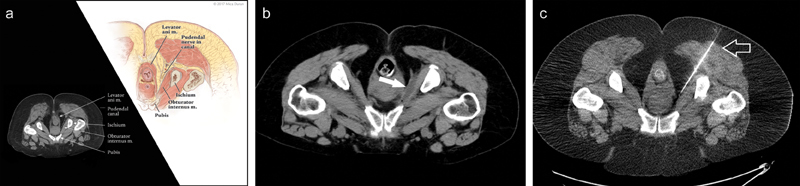
(
a
) Relevant planning landmarks for intervention to the pudendal canal. Axial CT scan from diagnostic pudendal nerve injection procedure (
left
) and corresponding anatomical landmarks (
right
). (
b
) Single axial postprocedure CT image from a pudendal nerve infiltration, demonstrating fluid in the pudendal canal (
arrow
). (
c
) Corresponding image from the subsequent cryoablation procedure, demonstrating placement of a 17-gauge cryoablation probe (
arrow
) in the ischiorectal fat adjacent to the nerve.
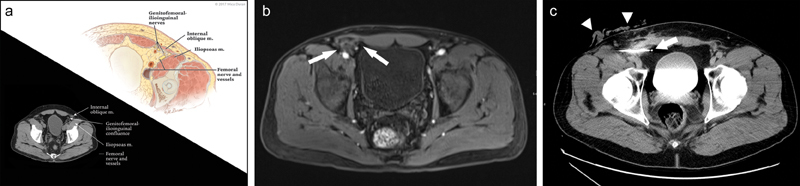
(
a
) Relevant planning landmarks for intervention in the setting of refractory inguinodynia (
left
) and corresponding anatomical landmarks (
right
). (
b
) Preprocedural T1 fat-saturated axial MR image from a patient with longstanding inguinodynia demonstrates fibrosis and stranding about the ilioinguinal and genitofemoral nerves (
arrows
), deep to implanted mesh. (
c
) Corresponding intraprocedural CT image from a cryoneurolysis procedure, demonstrating placement of the cryoablation probe (
arrow
) and warm saline protecting the overlying skin (
arrowheads
).
Similar articles
-
Effects of relaxing therapies on patient's pain during percutaneous interventional radiology procedures.Ann Palliat Med. 2018 Oct;7(4):455-462. doi: 10.21037/apm.2018.07.02. Epub 2018 Jul 20. Ann Palliat Med. 2018. PMID: 30180736
-
[Radiology: from diagnostic tool to interventional procedures].Ned Tijdschr Geneeskd. 2011;155:A3069. Ned Tijdschr Geneeskd. 2011. PMID: 21447227 Dutch.
-
The management of peri- and postprocedural pain in interventional radiology: a narrative review.Pain Manag. 2017 Nov;7(6):523-535. doi: 10.2217/pmt-2017-0024. Epub 2017 Nov 10. Pain Manag. 2017. PMID: 29125398 Review.
-
The Utility of Peripheral Nerve Blocks in Interventional Radiology.AJR Am J Roentgenol. 2016 Oct;207(4):718-730. doi: 10.2214/AJR.16.16643. Epub 2016 Jul 6. AJR Am J Roentgenol. 2016. PMID: 27385059
-
Sedation and analgesia in interventional radiology: Where do we stand, where are we heading and why does it matter?Diagn Interv Imaging. 2019 Dec;100(12):753-762. doi: 10.1016/j.diii.2019.10.002. Epub 2019 Nov 6. Diagn Interv Imaging. 2019. PMID: 31706790
Cited by
-
Minimally Invasive Treatment Strategies for Metastatic Disease of the Skeleton: Current Concepts.Curr Oncol Rep. 2025 Jun 11. doi: 10.1007/s11912-025-01696-w. Online ahead of print. Curr Oncol Rep. 2025. PMID: 40498266 Review. No abstract available.
References
-
- Kurup A N, Morris J M, Callstrom M R. Ablation of musculoskeletal metastases. AJR Am J Roentgenol. 2017;209(04):713–721. - PubMed
-
- Patel I J, Pirasteh A, Passalacqua M A et al.Palliative procedures for the interventional oncologist. AJR Am J Roentgenol. 2013;201(04):726–735. - PubMed
-
- Wallace A N, McWilliams S R, Connolly S E et al.Percutaneous image-guided cryoablation of musculoskeletal metastases: pain palliation and local tumor control. J Vasc Interv Radiol. 2016;27(12):1788–1796. - PubMed
-
- Greenwood T J, Wallace A, Friedman M V, Hillen T J, Robinson C G, Jennings J W. Combined ablation and radiation therapy of spinal metastases: a novel multimodality treatment approach. Pain Physician. 2015;18(06):573–581. - PubMed
