

Four-dimensional Plan Optimization for the Treatment of Lung Tumors Using Pencil-beam Scanning Proton Radiotherapy
- PMID: 30402360
- PMCID: PMC6200439
- DOI: 10.7759/cureus.3192
Four-dimensional Plan Optimization for the Treatment of Lung Tumors Using Pencil-beam Scanning Proton Radiotherapy
Abstract
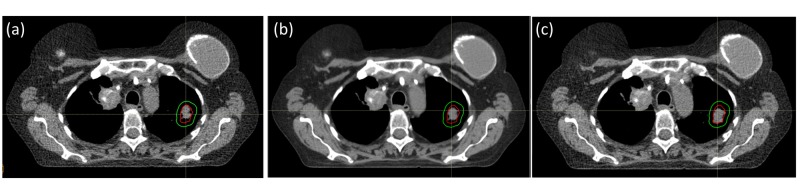
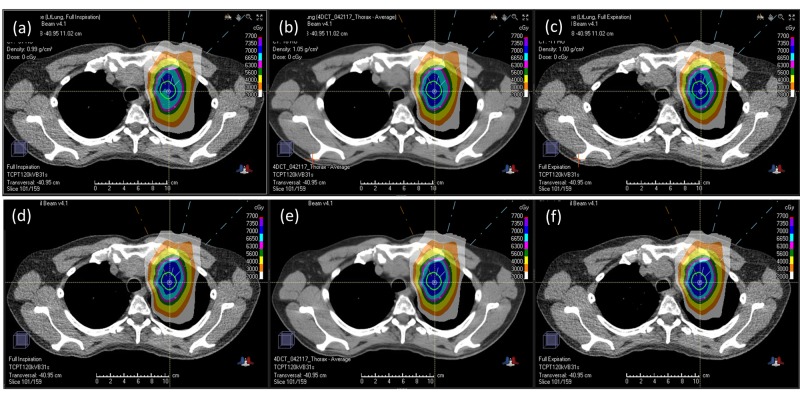
Purpose This study aimed to evaluate the effectiveness of four-dimensional (4D) robust optimization for proton pencil-beam scanning (PBS) treatment of lung tumors. Patients and methods In seven patients with lung cancer, proton beam therapy was planned using 4D robust optimization over 4D computed tomography (CT) data sets. The gross target volume (GTV) was contoured based on individual breathing phases, and a 5-mm expansion was used to generate the clinical target volume (CTV) for each phase. The 4D optimization was conducted directly on the 4D CT data set. The robust optimization settings included a CT Hounsfield unit (HU) uncertainty of 4% and a setup uncertainty of 5 mm to obtain the CTV. Additional target dose objectives such as those for the internal target volume (ITV) as well as the organ-at-risk (OAR) dose requirements were placed on the average CT. For comparison, three-dimensional (3D) robust optimization was also performed on the average CT. An additional verification 4D CT was performed to verify plan robustness against inter-fractional variations. Results Target coverages were generally higher for 4D optimized plans. The difference was most pronounced for ITV V70Gy when evaluating individual breathing phases. The 4D optimized plans were shown to be able to maintain the ITV coverage at full prescription, while 3D optimized plans could not. More importantly, this difference in ITV V70Gy between the 4D and 3D optimized plans was also consistently observed when evaluating the verification 4D CT, indicating that the 4D optimized plans were more robust against inter-fractional variations. Less difference was seen between the 4D and 3D optimized plans in the lungs criteria: V5Gy and V20Gy. Conclusion The proton PBS treatment plans optimized directly on the 4D CT were shown to be more robust when compared to those optimized on a regular 3D CT. Robust 4D optimization can improve the target coverage for the proton PBS lung treatments.
Keywords: 4d robust optimization; interplay effect; proton pbs treatment; robust optimization.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures



References
-
- Cancer statistics, 2017. Siegel RL, Miller KD, Jemal A. CA Cancer J Clin. 2017;67:7–30. - PubMed
LinkOut - more resources
Full Text Sources