

Improving survival after an emergency resuscitative thoracotomy: a 5-year review of the Trauma Quality Improvement Program
- PMID: 30402559
- PMCID: PMC6203136
- DOI: 10.1136/tsaco-2018-000201
Improving survival after an emergency resuscitative thoracotomy: a 5-year review of the Trauma Quality Improvement Program
Abstract
Background: Advancement in trauma care has led to the evolution of emergency resuscitative thoracotomy (ERT) for the revival of trauma patients. We now have more precise understanding of selecting suitable patients for achieving optimal outcomes. The aim of our study was to analyze the utilization and survival trends during the past 5 years, as well as factors that influence survival after ERT.
Methods: A 5-year (2010-2014) analysis of all trauma patients ≥18 years who underwent ERT in the American College of Surgeons Trauma Quality Improvement Program. Outcome measures were utilization rates and survival trends after ERT during the 5-year period. Regression analysis was performed.
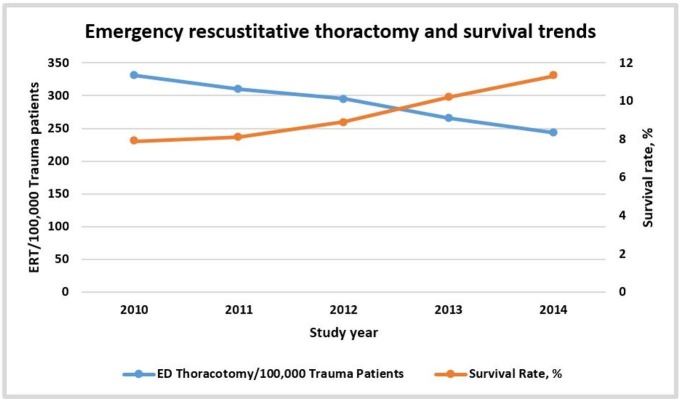
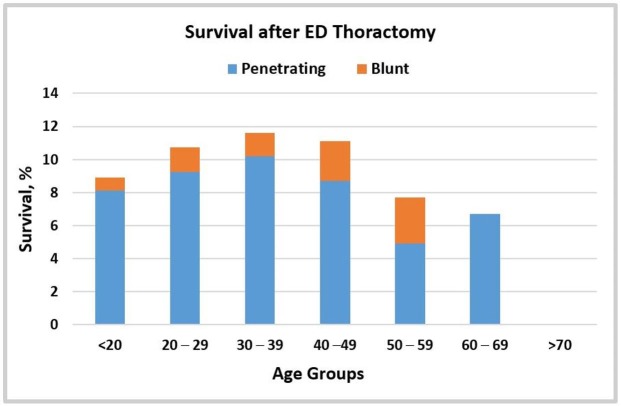
Results: 2229 patients underwent ERT, mean age was 37±17 years, 81% were male. Overall 56% patients had penetrating mechanism, location of major injury was thorax in 48, and 71% had signs of life (SOL) on arrival. The overall survival rate was 9.6%. From 2010-2014 ERT utilization has decreased from 331/100 000 to 243/100 000 trauma admissions (p=0.002) and the survival rate has improved from 7.9% to 11.3% (p<0.001). On regression, the independent predictors of survival were penetrating mechanism, age<60 years, SOL on arrival, no prehospital CPR and ISS. No patient aged >60 years with a blunt mechanism of injury (MOI) survived, and there were no survivors above the age of 70 years, regardless of injury mechanism.
Discussion: Utilization of ERT has been decreased during the study period along with improved survival rates. The results of our study demonstrate that performing ERT on patients aged >60 years with a blunt MOI or on any patient aged ≥70 years, regardless of MOI, is futile and should be avoided.
Level of evidence: Level III, prognostic studies.
Keywords: emergency resuscitative thoracotomy; trauma; trends.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Prevention CfDCa. FastStats - leading causes of death: Centers for Disease Control and Prevention, 2017.
-
- Rhee PM, Acosta J, Bridgeman A, Wang D, Jordan M, Rich N. Survival after emergency department thoracotomy: review of published data from the past 25 years. J Am Coll Surg 2000;190:288–98. - PubMed
-
- Hopson LR, Hirsh E, Delgado J, Domeier RM, Krohmer J, McSwain NE, Weldon C, Friel M, Hoyt DB. National Association of EMS Physicians Standards and Clinical Practice Committee. Guidelines for withholding or termination of resuscitation in prehospital traumatic cardiopulmonary arrest. J Am Coll Surg 2003;196:475–81. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous