

Clinical Pharmacology of Fast-Acting Insulin Aspart Versus Insulin Aspart Measured as Free or Total Insulin Aspart and the Relation to Anti-Insulin Aspart Antibody Levels in Subjects with Type 1 Diabetes Mellitus
- PMID: 30402720
- PMCID: PMC6451708
- DOI: 10.1007/s40262-018-0718-6
Clinical Pharmacology of Fast-Acting Insulin Aspart Versus Insulin Aspart Measured as Free or Total Insulin Aspart and the Relation to Anti-Insulin Aspart Antibody Levels in Subjects with Type 1 Diabetes Mellitus
Abstract
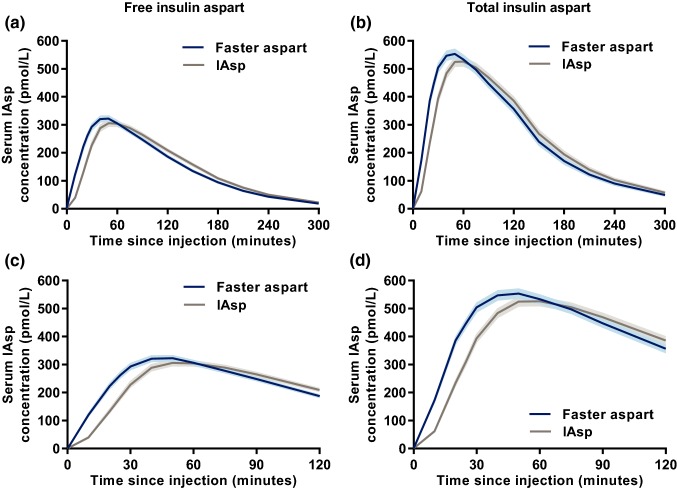
Background: Fast-acting insulin aspart (faster aspart) is an ultra-fast-acting formulation of insulin aspart (IAsp). This post hoc analysis investigated the pharmacokinetics of faster aspart versus IAsp, measured as free or total IAsp, and the relationship between anti-IAsp antibodies and the pharmacokinetics/pharmacodynamics of faster aspart and IAsp.
Methods: Free and total IAsp concentrations and anti-IAsp antibodies were determined in adults with type 1 diabetes mellitus receiving subcutaneous faster aspart and/or IAsp in four single-dose clinical pharmacology trials (n = 175) and a 26-week phase IIIa trial (n = 1040). Pharmacodynamics were assessed by euglycaemic clamp or meal test, respectively.
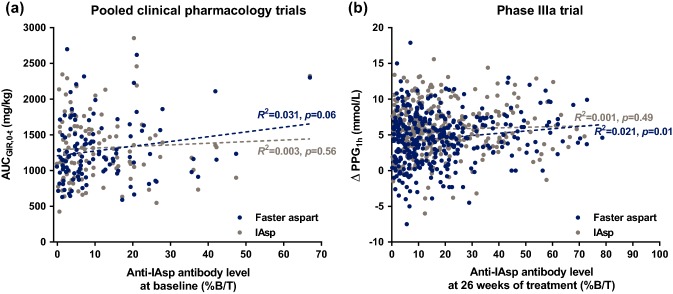
Results: The pharmacokinetic profile was left-shifted and early exposure was greater with faster aspart versus IAsp independent of free or total IAsp assay. The faster aspart-IAsp difference in the time to 50% of maximum IAsp concentration in the early part of the pharmacokinetic profile (tEarly 50 % Cmax) [95% confidence interval (CI)] was - 8.8 [- 10.0 to - 7.5] and - 7.6 [- 8.8 to - 6.4] min for free and total IAsp, respectively. The faster aspart/IAsp ratio for the area under the concentration-time curve (AUC) for IAsp from time zero to 30 min (AUCIAsp,0-30 min) [95% CI] was 1.88 [1.74-2.04] and 1.77 [1.64-1.90] for free and total IAsp. Higher anti-IAsp antibody levels were associated with a lower ratio of free/total IAsp for the total AUC for IAsp (AUCIAsp,0-t). Early glucose-lowering effect (AUC for the glucose infusion rate [GIR] from time zero to 60 min [AUCGIR,0-60 min]) was greater by 25-44% for faster aspart versus IAsp independent of anti-IAsp antibody levels. Total glucose-lowering effect (total AUC for GIR [AUCGIR,0-t]) in a clamp and 1-h postprandial glucose increment in a meal test appeared essentially unaffected by anti-IAsp antibodies.
Conclusions: Faster aspart provides accelerated pharmacokinetics versus IAsp regardless if based on free or total IAsp assay. Higher anti-IAsp antibodies increase total IAsp concentrations but do not influence faster aspart nor IAsp pharmacodynamics. CLINICALTRIALS.
Gov identifiers: NCT01618188, NCT02003677, NCT01934712, NCT02568280, NCT01831765.
Conflict of interest statement
Ethical approval and informed consent
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Conflict of interest
Hanne Haahr and Lars Erichsen are employees and shareholders of Novo Nordisk. Theis Gondolf is an employee of Novo Nordisk. Thomas R. Pieber has received research support from AstraZeneca and Novo Nordisk, has served in advisory panels for AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Novo Nordisk and Roche Diabetes Care, and is an employee of CBmed - Center for Biomarker Research in Medicine (a publically funded research centre). Chantal Mathieu serves or has served on advisory panels for Novo Nordisk, Sanofi, Merck Sharp and Dohme, Eli Lilly, Novartis, Bristol-Myers Squibb, AstraZeneca, Pfizer, Janssen Pharmaceuticals, Boehringer Ingelheim, Hanmi Pharmaceuticals, Roche Diagnostics, Medtronic, Mannkind, Intrexon, Dianax and UCB, and as a speaker for Novo Nordisk, Sanofi, Merck Sharp and Dohme, Eli Lilly, Boehringer Ingelheim, AstraZeneca and Novartis. Financial compensation for these activities has been received by KU Leuven. KU Leuven has received research support for Chantal Mathieu from Medtronic, Novo Nordisk, Sanofi, Merck Sharp and Dohme, Eli Lilly, Roche Diagnostics, Abbott, Intrexon and Novartis. Tim Heise is a shareholder of Profil, which has received research funds from Adocia, Boehringer Ingelheim, Dance Pharmaceuticals, Eli Lilly, Johnson & Johnson, MedImmune, Merck Sharp and Dohme, Mylan, Nordic Bioscience, Novo Nordisk, Poxel, Roche Diagnostics, Saniona, Sanofi, Senseonics and Zealand Pharma. In addition, Tim Heise is member of advisory panels for Novo Nordisk and Mylan and received speaker honoraria and travel grants from Dexcom, Eli Lilly, Mylan, Novo Nordisk, Sanofi and Zealand Pharma. Masanari Shiramoto has no conflicts of interest to declare.
Data availability
Figures

References
-
- Arnqvist H, Olsson PO, von Schenck H. Free and total insulin as determined after precipitation with polyethylene glycol: analytical characteristics and effects of sample handling and storage. Clin Chem. 1987;33:93–96. - PubMed
-
- Sapin R. Insulin assays: previously known and new analytical features. Clin Lab. 2003;49:113–121. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
