

Neoadjuvant (Chemo)radiotherapy With Total Mesorectal Excision Only Is Not Sufficient to Prevent Lateral Local Recurrence in Enlarged Nodes: Results of the Multicenter Lateral Node Study of Patients With Low cT3/4 Rectal Cancer
- PMID: 30403572
- PMCID: PMC6366816
- DOI: 10.1200/JCO.18.00032
Neoadjuvant (Chemo)radiotherapy With Total Mesorectal Excision Only Is Not Sufficient to Prevent Lateral Local Recurrence in Enlarged Nodes: Results of the Multicenter Lateral Node Study of Patients With Low cT3/4 Rectal Cancer
Abstract
Purpose: Improvements in magnetic resonance imaging (MRI), total mesorectal excision (TME) surgery, and the use of (chemo)radiotherapy ([C]RT) have improved local control of rectal cancer; however, we have been unable to eradicate local recurrence (LR). Even in the face of TME and negative resection margins (R0), a significant proportion of patients with enlarged lateral lymph nodes (LLNs) suffer from lateral LR (LLR). Japanese studies suggest that the addition of an LLN dissection (LLND) could reduce LLR. This multicenter pooled analysis aims to ascertain whether LLNs actually pose a problem and whether LLND results in fewer LLRs.
Patients and methods: Data from 1,216 consecutive patients with cT3/T4 rectal cancers up to 8 cm from the anal verge who underwent surgery in a 5-year period were collected. LLND was performed in 142 patients (12%). MRIs were re-evaluated with a standardized protocol to assess LLN features.
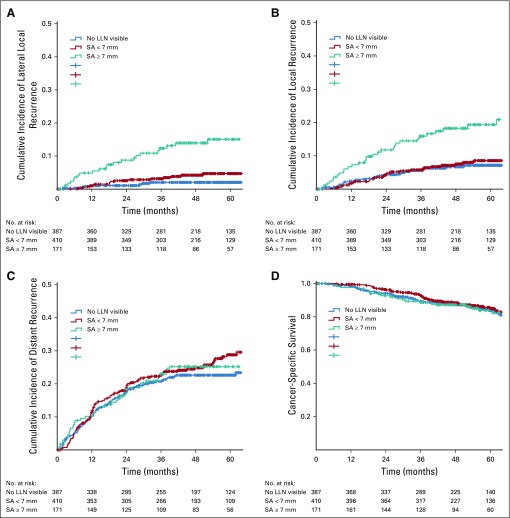
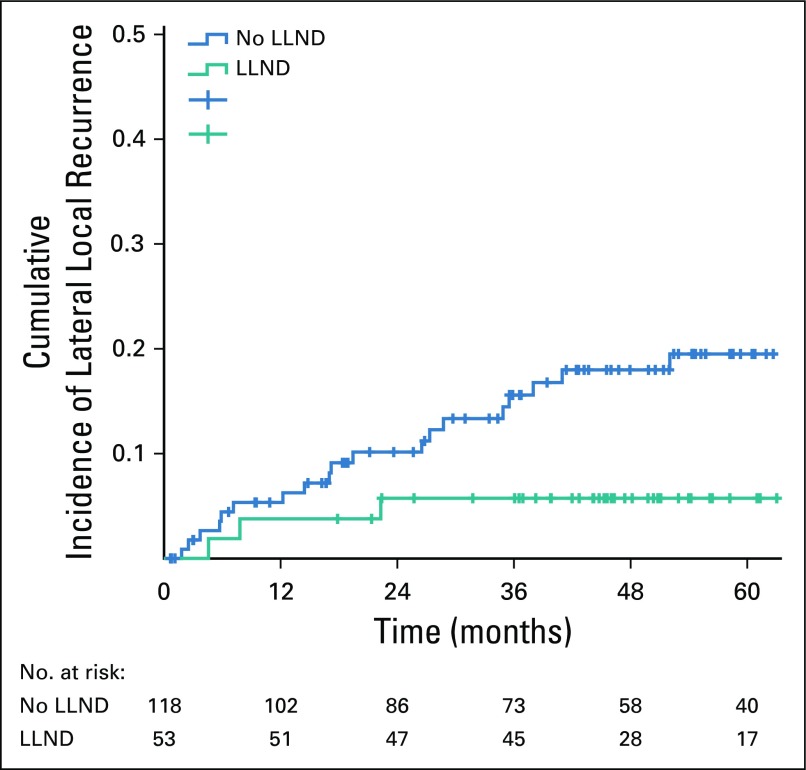
Results: On pretreatment MRI, 703 patients (58%) had visible LLN, and 192 (16%) had a short axis of at least 7 mm. One hundred eight patients developed LR (5-year LR rate, 10.0%), of which 59 (54%) were LLRs (5-year LLR rate, 5.5%). After multivariable analyses, LLNs with a short axis of at least 7 mm resulted in a significantly higher risk of LLR (hazard ratio, 2.060; P = .045) compared with LLNs of less than 7 mm. In patients with LLNs at least 7 mm, (C)RT plus TME plus LLND resulted in a 5-year LLR of 5.7%, which was significantly lower than that in patients who underwent (C)RT plus TME (5-year LLR, 19.5%; P = .042).
Conclusion: LLR is still a significant problem after (C)RT plus TME in LLNs with a short axis at least 7 mm on pretreatment MRI. The addition of LLND results in a significantly lower LLR rate.
Figures
Comment in
-
[Lateral pelvic lymph nodes in locally advanced rectal carcinoma-an underestimated site of recurrence?].Strahlenther Onkol. 2019 Jun;195(6):576-578. doi: 10.1007/s00066-019-01447-4. Strahlenther Onkol. 2019. PMID: 30859255 German. No abstract available.
-
Gastrointestinal Cancers: Fine-Tuning the Management of Rectal, Esophageal, and Pancreas Cancers.Int J Radiat Oncol Biol Phys. 2019 Sep 1;105(1):1-10. doi: 10.1016/j.ijrobp.2019.04.037. Int J Radiat Oncol Biol Phys. 2019. PMID: 31422802 Free PMC article. No abstract available.
References
-
- Heald RJ, Ryall RD. Recurrence and survival after total mesorectal excision for rectal cancer. Lancet. 1986;1:1479–1482. - PubMed
-
- Beets-Tan RGH, Beets GL, Vliegen RFA, et al. Accuracy of magnetic resonance imaging in prediction of tumour-free resection margin in rectal cancer surgery. Lancet. 2001;357:497–504. - PubMed
-
- Taylor FG, Quirke P, Heald RJ, et al. Preoperative magnetic resonance imaging assessment of circumferential resection margin predicts disease-free survival and local recurrence: 5-year follow-up results of the MERCURY study. J Clin Oncol. 2014;32:34–43. - PubMed
-
- Beets-Tan RGH, Lambregts DMJ, Maas M, et al. Magnetic resonance imaging for clinical management of rectal cancer: Updated recommendations from the 2016 European Society of Gastrointestinal and Abdominal Radiology (ESGAR) consensus meeting. Eur Radiol. 2018;28:1465–1475. [Erratum: Eur Radiol 28:2711, 2018] - PMC - PubMed
-
- Swedish Rectal Cancer Trial. Cedermark B, Dahlberg M, et al. Improved survival with preoperative radiotherapy in resectable rectal cancer. N Engl J Med. 1997;336:980–987. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
