

Menopausal Hormone Therapy use and breast cancer risk by receptor subtypes: Results from the New South Wales Cancer Lifestyle and EvaluAtion of Risk (CLEAR) study
- PMID: 30403669
- PMCID: PMC6221262
- DOI: 10.1371/journal.pone.0205034
Menopausal Hormone Therapy use and breast cancer risk by receptor subtypes: Results from the New South Wales Cancer Lifestyle and EvaluAtion of Risk (CLEAR) study
Abstract
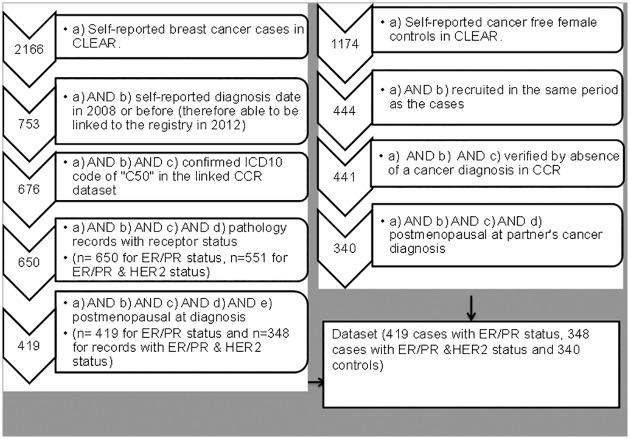
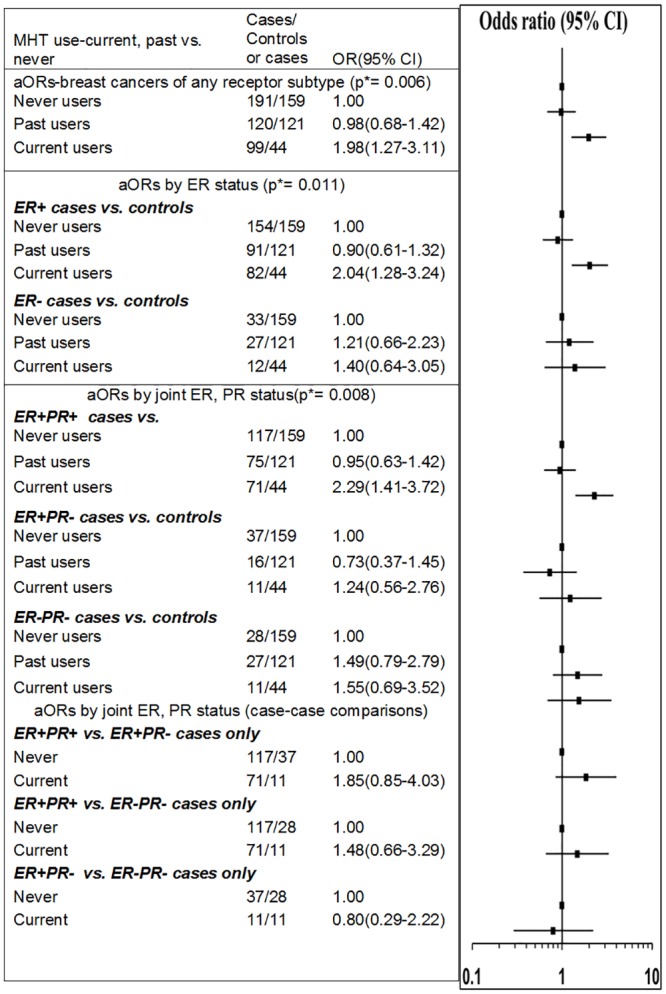
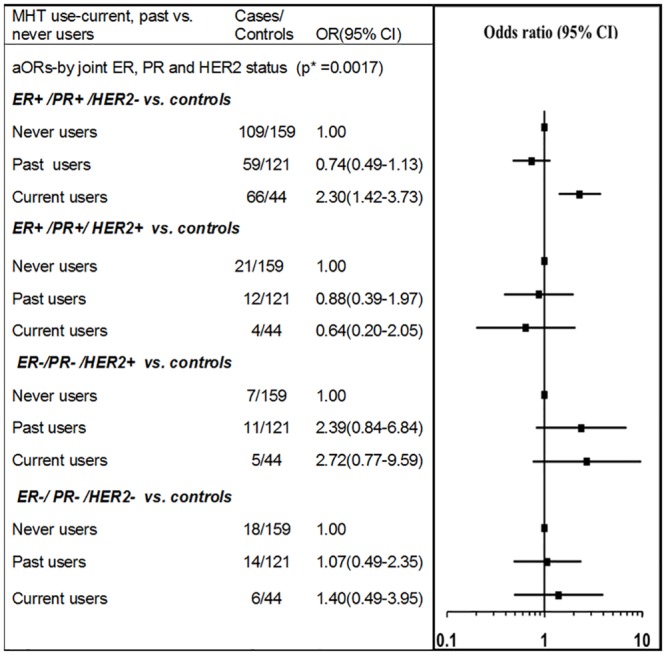
Breast cancer risk is increased with current Menopausal Hormone Therapy (MHT) use, with higher risks reported for ER+ (Estrogen Receptor positive), and ER+/PR+ (Estrogen and Progesterone Receptor positive) breast cancers than those of ER- and ER-/PR- status, respectively. There is limited evidence to suggest MHT use is associated with the specific subtype characterised as ER+/PR+/HER2- (Estrogen and Progesterone Receptor positive and Human Epidermal growth factor Receptor2 negative) status. This study aims to investigate the MHT-breast cancer relationship for breast cancer tumor receptor subtypes defined by ER expression alone, by ER and PR expression only and by joint expression of ER, PR, and HER2. Analyses compared 399 cancer registry-verified breast cancer cases with receptor status information and 324 cancer-free controls. We used multinomial logistic regression to estimate adjusted odds ratios (aORs) and 95% Confidence Intervals (CI) for current and past versus never MHT use, for subgroups defined by tumor receptor expression. Current, but not past, use of MHT was associated with an elevated risk of ER+ breast cancer (aOR = 2.04, 95%CI: 1.28-3.24) and ER+/PR+ breast cancer (aOR = 2.29, 1.41-3.72). Current MHT use was also associated with an elevated risk of the ER+/PR+/HER2- subtype (aOR = 2.30, 1.42-3.73). None of the other subtypes based on ER, ER/PR or ER/PR/HER2 expression were significantly associated with current MHT use in this analysis. Current, but not past, use of MHT increases the risk of breast cancer, with consistently higher risks reported for ER+ and ER+/PR+ subtypes and mounting evidence regarding the specific ER+/PR+/HER2- subtype. Our findings contribute to quantification of the effects of MHT, and support efforts to articulate the receptor-mediated mechanisms by which MHT increases the risk of breast cancer.
Conflict of interest statement
The authors have declared that no competing interests exist. KC is co-principal investigator of an investigator-initiated trial of cytology and primary HPV screening in Australia (Compass; ACTRN12613001207707 and NCT02328872), which is conducted and funded by the Victorian Cytology Service (VCS), a government-funded health promotion charity. VCS has received equipment and a funding contribution for the Compass trial from Roche Molecular Systems and Ventana USA. KC is also an investigator for Compass in New Zealand (Compass NZ; ACTRN12614000714684), which is conducted and funded by Diagnostic Medlab (DML), now Auckland District Health Board. DML received an equipment and funding contribution for the Compass trial from Roche Molecular Systems. However neither KC nor her institution on her behalf (Cancer Council NSW) receive direct or indirect funding from industry for Compass Australia or NZ or any other project. This does not alter the authors’ adherence to PLOS ONE policies on sharing data and materials.
Figures
Similar articles
-
Parity, hormones and breast cancer subtypes - results from a large nested case-control study in a national screening program.Breast Cancer Res. 2017 Jan 23;19(1):10. doi: 10.1186/s13058-016-0798-x. Breast Cancer Res. 2017. PMID: 28114999 Free PMC article.
-
Reproductive characteristics, menopausal status, race and ethnicity, and risk of breast cancer subtypes defined by ER, PR and HER2 status: the Breast Cancer Etiology in Minorities study.Breast Cancer Res. 2024 May 31;26(1):88. doi: 10.1186/s13058-024-01834-5. Breast Cancer Res. 2024. PMID: 38822357 Free PMC article.
-
CORRELATION BETWEEN CLINICAL PATHOLOGY OF LUMINAL B BREAST CANCER AND DETERMINATION OF ESTROGEN RECEPTOR, PROGESTERONE RECEPTOR AND HER2 EXPRESSION COMBINED WITH NUCLEAR MORPHOLOGY.J Biol Regul Homeost Agents. 2015 Jul-Sep;29(3):579-87. J Biol Regul Homeost Agents. 2015. PMID: 26403396 Clinical Trial.
-
Hormone receptors in breast cancer: An update on the uncommon subtypes.Pathol Res Pract. 2023 Oct;250:154791. doi: 10.1016/j.prp.2023.154791. Epub 2023 Sep 3. Pathol Res Pract. 2023. PMID: 37672851 Review.
-
Research progress on estrogen receptor-positive/progesterone receptor-negative breast cancer.Transl Oncol. 2025 Jun;56:102387. doi: 10.1016/j.tranon.2025.102387. Epub 2025 Apr 14. Transl Oncol. 2025. PMID: 40222338 Free PMC article. Review.
Cited by
-
Menopausal hormone therapy and incidence, mortality, and survival of breast cancer subtypes: a prospective cohort study.Breast Cancer Res. 2024 Nov 4;26(1):151. doi: 10.1186/s13058-024-01897-4. Breast Cancer Res. 2024. PMID: 39497219 Free PMC article.
-
Early-life body mass index and risks of breast, endometrial, and ovarian cancers: a dose-response meta-analysis of prospective studies.Br J Cancer. 2022 Mar;126(4):664-672. doi: 10.1038/s41416-021-01625-1. Epub 2021 Nov 12. Br J Cancer. 2022. PMID: 34773099 Free PMC article.
-
Relationship of established risk factors with breast cancer subtypes.Cancer Med. 2021 Sep;10(18):6456-6467. doi: 10.1002/cam4.4158. Epub 2021 Aug 31. Cancer Med. 2021. PMID: 34464510 Free PMC article.
-
Comparison of pyrotinib or lapatinib with chemotherapy for patients with HER2 positive breast cancer after first-line treatment failure: a retrospective study.Am J Transl Res. 2021 Sep 15;13(9):10863-10870. eCollection 2021. Am J Transl Res. 2021. PMID: 34650767 Free PMC article.
-
Hormone-Replacement Therapy and Its Association with Breast Cancer Subtypes: A Large Retrospective Cohort Study.Int J Womens Health. 2021 Dec 3;13:1207-1216. doi: 10.2147/IJWH.S311696. eCollection 2021. Int J Womens Health. 2021. PMID: 34887685 Free PMC article.
References
-
- Rastelli F, Crispino S. Factors predictive of response to hormone therapy in breast cancer. Tumori 2008; 94: 370–383. - PubMed
-
- Collaborative Group on Hormonal Factors in Breast Cancer. Menarche, menopause, and breast cancer risk: individual participant meta-analysis, including 118 964 women with breast cancer from 117 epidemiological studies. Lancet Oncol. 2012;13: 1141–1151. 10.1016/S1470-2045(12)70425-4 - DOI - PMC - PubMed
-
- Colditz GA, Rosner BA, Chen WY, Holmes MD, Hankinson SE. Risk Factors for Breast Cancer according to Estrogen and Progesterone Receptor Status. J Natl Cancer Inst. 2004; 96: 218–228. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
