

Comparison of FIB-4 and transient elastography in evaluating liver fibrosis of chronic hepatitis C subjects in community
- PMID: 30403744
- PMCID: PMC6221348
- DOI: 10.1371/journal.pone.0206947
Comparison of FIB-4 and transient elastography in evaluating liver fibrosis of chronic hepatitis C subjects in community
Abstract
Background and aim: The role of non-invasive methods to evaluate fibrosis severity of chronic hepatitis C (CHC) subjects in community needs to be explored. This study investigated FIB-4 and transient elastography (TE) in staging liver fibrosis of CHC subjects in community.
Methods: A total of 905 subjects who were positive for anti-HCV antibody from five districts of Tainan City of Taiwan were invited to participate in surveillance activities for CHC. FIB-4 and TE were measured for each participant.
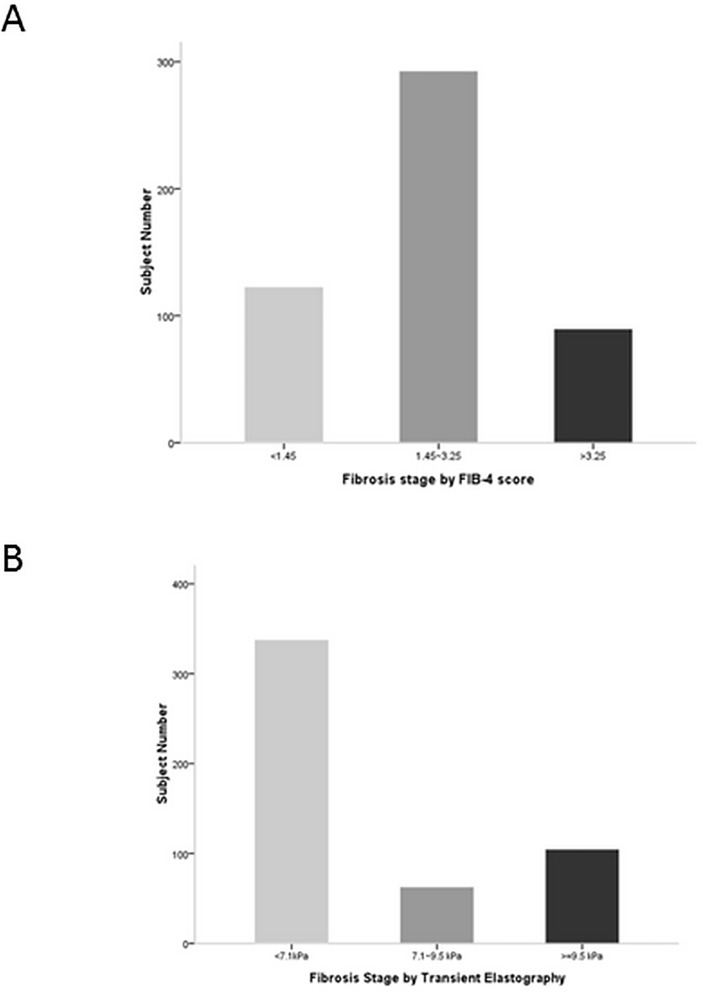
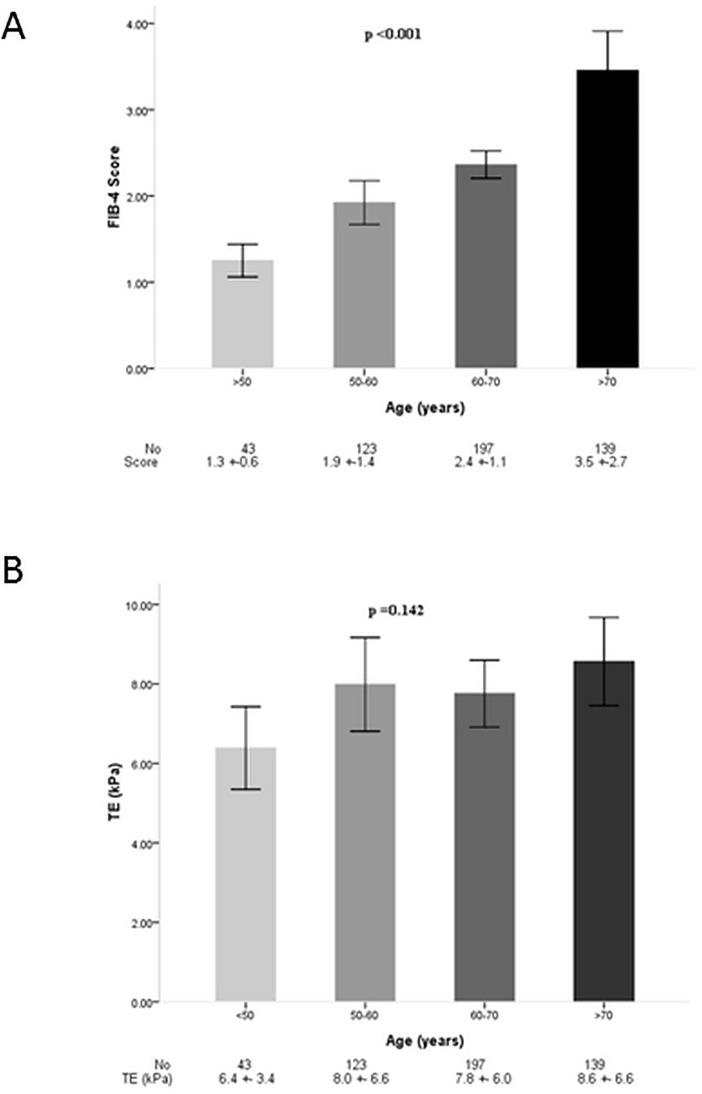
Results: A total of 502 subjects with detectable HCV RNA and valid TE were enrolled. The distribution of FIB-4 and TE values differed markedly. Both methods exhibited a strongest correlation in subjects with at age 50~60 years (r = 0.655, p <0.001). FIB-4 score increased proportionally with age (p <0.001), but TE did not (p = 0.142). The intraclass correlation efficient of both methods was 0.255 (p <0.001). Subjects with TE defined advanced fibrosis exhibited younger age, higher BMI, higher platelet count, lower FIB-4 score, higher incidence of fatty liver and splenomegaly, and higher controlled attenuation parameter value than those defined by FIB-4. By multivariate logistic regression analysis, higher ALT levels, higher incidence of fatty liver, and presence of splenomegaly were the independent factors associated with advanced fibrosis defined by TE rather than defined by FIB-4.
Conclusions: FIB-4 and TE defined different distribution of fibrosis stages in same HCV population. FIB-4 was deeply influenced by age whereas TE was not. TE had the advantages over than FIB-4 in strong association with splenomegaly and in detecting the role of non-alcoholic fatty liver disease in advanced fibrosis.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Direct antiviral agent treatment of chronic hepatitis C results in rapid regression of transient elastography and fibrosis markers fibrosis-4 score and aspartate aminotransferase-platelet ratio index.Liver Int. 2017 Mar;37(3):369-376. doi: 10.1111/liv.13256. Epub 2016 Nov 3. Liver Int. 2017. PMID: 27678216
-
The applicability of non-invasive methods for assessing liver fibrosis in hemodialysis patients with chronic hepatitis C.PLoS One. 2020 Nov 20;15(11):e0242601. doi: 10.1371/journal.pone.0242601. eCollection 2020. PLoS One. 2020. PMID: 33216807 Free PMC article.
-
Correlation of transient elastography with APRI and FIB-4 in a cohort of patients with congenital bleeding disorders and HCV or HIV/HCV coinfection.Haemophilia. 2010 Sep 1;16(5):778-85. doi: 10.1111/j.1365-2516.2010.02204.x. Epub 2010 Mar 15. Haemophilia. 2010. PMID: 20331759
-
Clinical application of transient elastography in patients with chronic viral hepatitis receiving antiviral treatment.Liver Int. 2015 Apr;35(4):1103-15. doi: 10.1111/liv.12628. Epub 2014 Jul 19. Liver Int. 2015. PMID: 24976523 Review.
-
Accuracy of blood-based biomarkers for staging liver fibrosis in chronic liver disease: A systematic review supporting the AASLD Practice Guideline.Hepatology. 2025 Jan 1;81(1):358-379. doi: 10.1097/HEP.0000000000000842. Epub 2024 Mar 15. Hepatology. 2025. PMID: 38489517
Cited by
-
Non-invasive tests for the prediction of primary hepatocellular carcinoma.World J Gastroenterol. 2020 Jun 28;26(24):3326-3343. doi: 10.3748/wjg.v26.i24.3326. World J Gastroenterol. 2020. PMID: 32655261 Free PMC article. Review.
-
Significant Correlation Between Grip Strength and m2bpgi in Patients with Chronic Liver Diseases.J Clin Med. 2019 Sep 1;8(9):1359. doi: 10.3390/jcm8091359. J Clin Med. 2019. PMID: 31480612 Free PMC article.
-
Longitudinal assessment of liver stiffness by transient elastography for chronic hepatitis C patients.World J Clin Cases. 2022 Jun 16;10(17):5566-5576. doi: 10.12998/wjcc.v10.i17.5566. World J Clin Cases. 2022. PMID: 35979107 Free PMC article.
-
Real-world single-center experience with direct-acting antivirals for improvement of the liver fibrosis after chronic hepatitis C treatment.Antivir Chem Chemother. 2020 Jan-Dec;28:2040206620974835. doi: 10.1177/2040206620974835. Antivir Chem Chemother. 2020. PMID: 33215505 Free PMC article.
-
Role of Lymphotoxin-α Gene Polymorphism in Hepatitis C Virus-Related Chronic Liver Disorders.Infect Drug Resist. 2021 May 25;14:1921-1930. doi: 10.2147/IDR.S306879. eCollection 2021. Infect Drug Resist. 2021. PMID: 34079302 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
