

Using linked electronic health records to report healthcare-associated infections
- PMID: 30403746
- PMCID: PMC6221334
- DOI: 10.1371/journal.pone.0206860
Using linked electronic health records to report healthcare-associated infections
Abstract
Background: Reporting of strategic healthcare-associated infections (HCAIs) to Public Health England is mandatory for all acute hospital trusts in England, via a web-based HCAI Data Capture System (HCAI-DCS).
Aim: Investigate the feasibility of automating the current, manual, HCAI reporting using linked electronic health records (linked-EHR), and assess its level of accuracy.
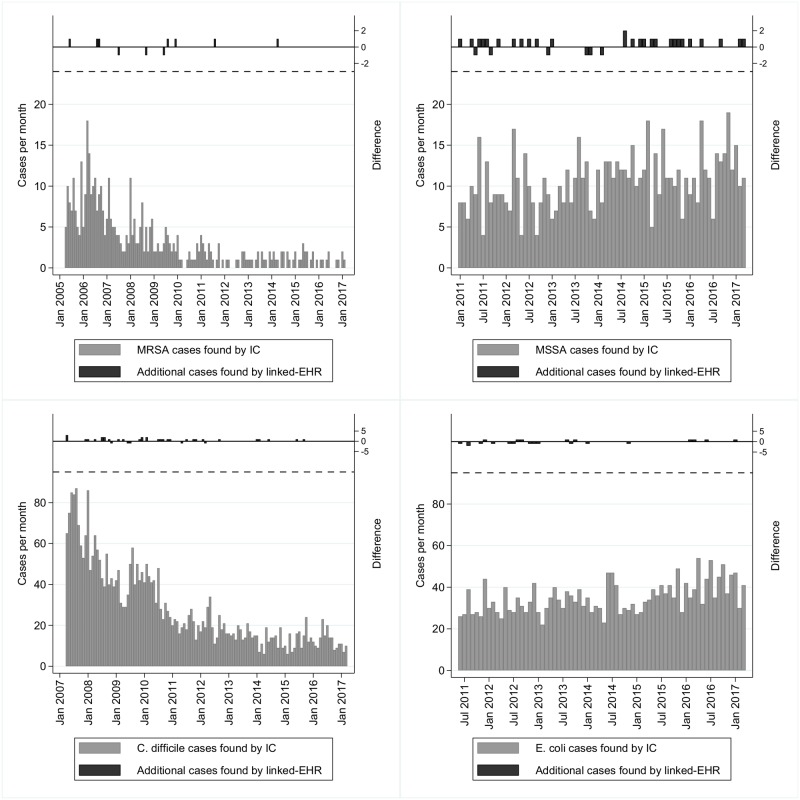
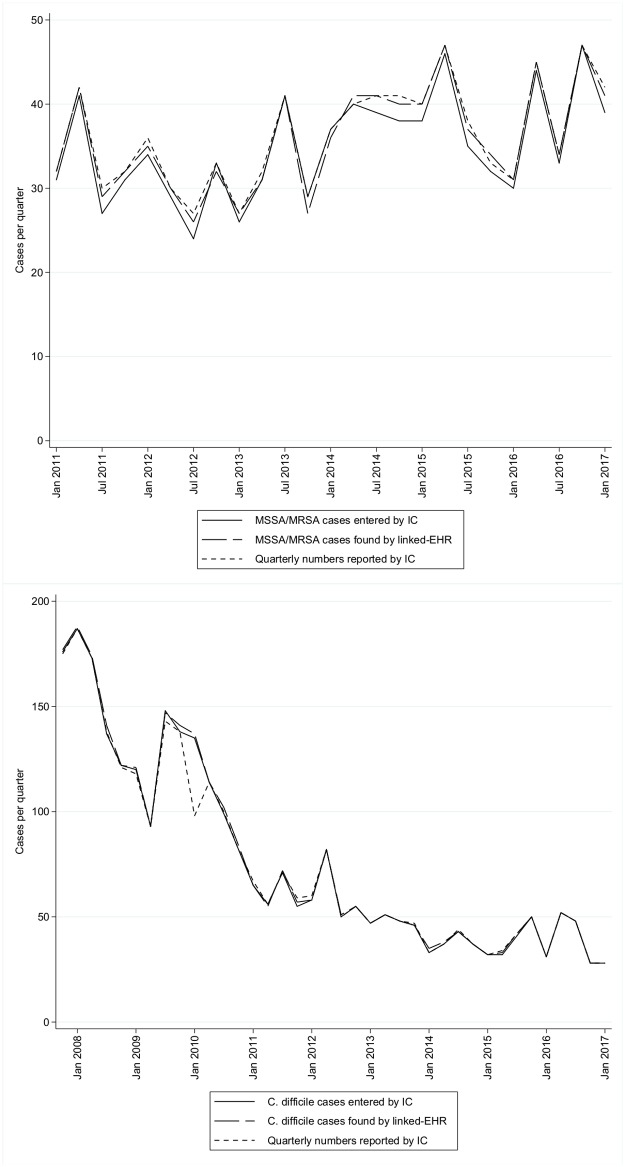
Methods: All data previously submitted through the HCAI-DCS by the Oxford University Hospitals infection control (IC) team for methicillin-resistant and methicillin-susceptible Staphylococcus aureus (MRSA, MSSA), Clostridium difficile, and Escherichia coli, through March 2017 were downloaded and compared to outputs created from linked-EHR, with detailed comparisons between 2013-2017.
Findings: Total MRSA, MSSA, E. coli and C. difficile cases entered by the IC team vs linked-EHR were 428 vs 432, 795 vs 816, 2454 vs 2450 and 3365 vs 3393 respectively. From 2013-2017, most discrepancies (32/37 (86%)) were likely due to IC recording errors. Patient and specimen identifiers were completed for >98% of cases by both methods, with very high agreement (>97%). Fields relating to the patient at the time the specimen was taken were complete to a similarly high level (>99% IC, >97% linked-EHR), and agreement was fairly good (>80%) except for the main and treatment specialties (57% and 54% respectively) and the patient category (55%). Optional, organism-specific data-fields were less complete, by both methods. Where comparisons were possible, agreement was reasonably high (mostly 70-90%).
Conclusion: Basic factual information, such as demographic data, is almost-certainly better automated, and many other data fields can potentially be populated successfully from linked-EHR. Manual data collection is time-consuming and inefficient; automated electronic data collection would leave healthcare professionals free to focus on clinical rather than administrative work.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Public Health England. Mandatory enhanced MRSA, MSSA and Escherichia coli bacteraemia, and Clostridium difficile infection surveillance: Protocol version 4.0. Public Health England; 2016.
-
- Wilson AP, Kiernan M. Recommendations for surveillance priorities for healthcare-associated infections and criteria for their conduct. J Antimicrob Chemother. 2012;67 Suppl 1:i23–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
