

Impaired urinary concentration ability is a sensitive predictor of renal disease progression in Joubert syndrome
- PMID: 30403813
- PMCID: PMC7417010
- DOI: 10.1093/ndt/gfy333
Impaired urinary concentration ability is a sensitive predictor of renal disease progression in Joubert syndrome
Abstract
Background: Joubert syndrome (JS) is an inherited ciliopathy characterized by a complex midbrain-hindbrain malformation and multiorgan involvement. Renal disease, mainly juvenile nephronophthisis (NPH), was reported in 25-30% patients although only ∼18% had a confirmed diagnosis of chronic kidney disease (CKD). NPH often remains asymptomatic for many years, resulting in delayed diagnosis. The aim of the study was to identify a biomarker able to quantify the risk of progressive CKD in young children with JS.
Methods: Renal features were investigated in 93 Italian patients, including biochemical tests, ultrasound and 1-deamino-8D-arginine vasopressin test in children with reduced basal urine osmolality. A subset of patients was followed-up over time.
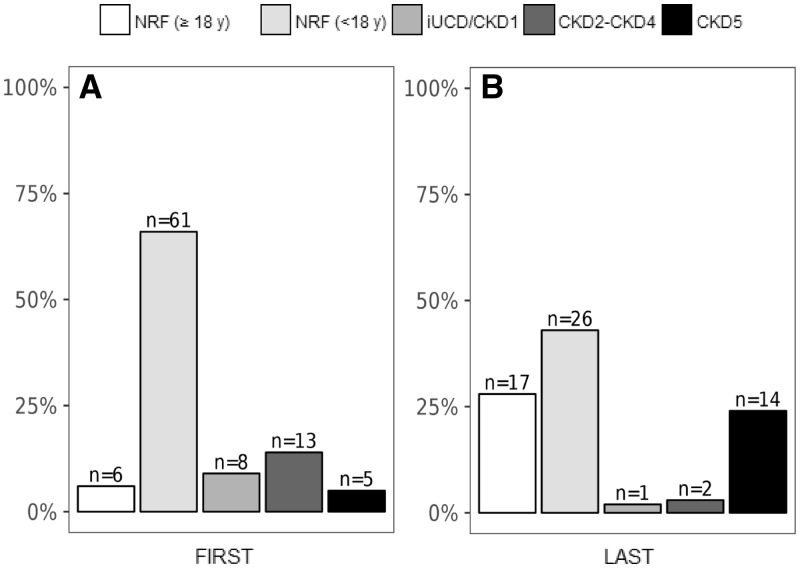
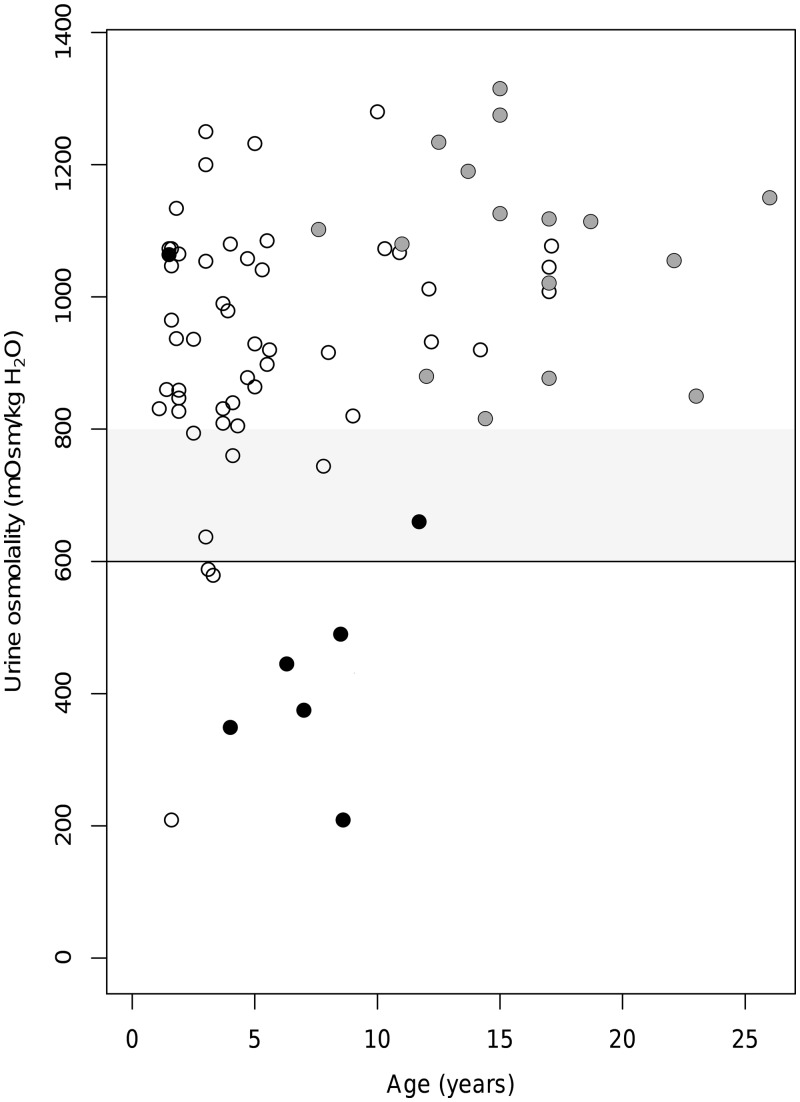
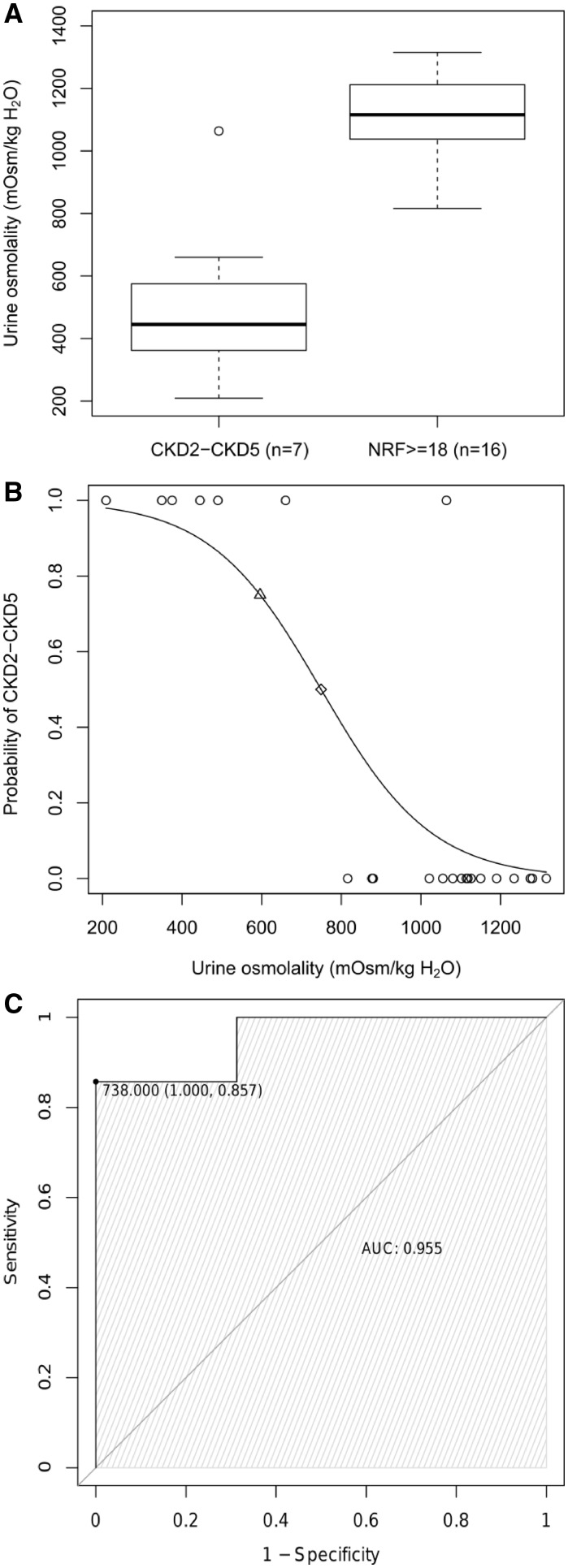
Results: At last examination, 27 of 93 subjects (29%) presented with CKD, ranging from isolated urinary concentration defect (UCD) to end-stage renal disease. Both normal and pathological urine osmolality levels remained stable over time, even when obtained at very early ages. Follow-up data showed that the probability of developing CKD can be modelled as a function of the urine osmolality value, exceeding 75% for levels <600 mOsm/kg H2O, and significantly increased in patients with an early diagnosis of isolated UCD.
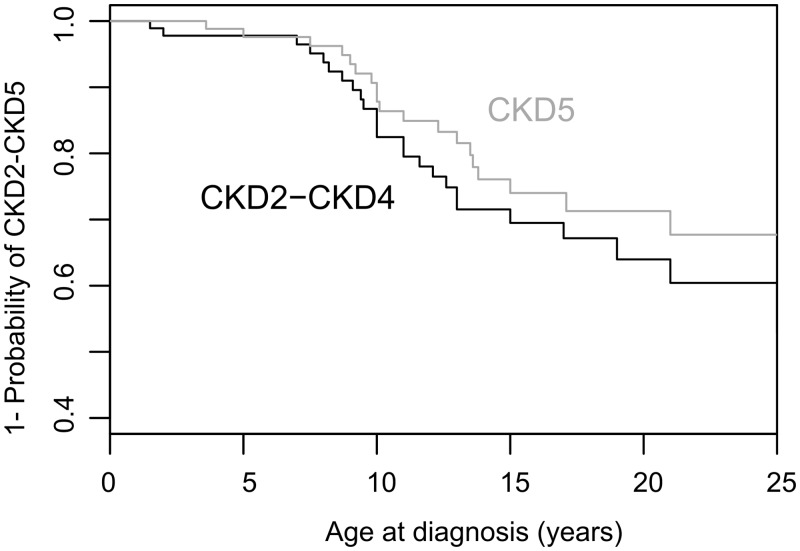
Conclusions: We conclude that the frequency of CKD in JS increases with age and is higher than previously reported. Urine osmolality represents an early sensitive quantitative biomarker of the risk of CKD progression.
Keywords: 1-deamino-8D-arginine vasopressin test; Joubert syndrome; early diagnosis; nephronophthisis; urine osmolality.
© The Author(s) 2018. Published by Oxford University Press on behalf of ERA-EDTA.
Figures
References
-
- Mitchison HM, Valente EM.. Motile and non-motile cilia in human pathology: from function to phenotypes. J Pathol 2017; 241: 294–309 - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
