

Pathogenesis of ANCA-Associated Pulmonary Vasculitis
- PMID: 30404109
- PMCID: PMC6343662
- DOI: 10.1055/s-0038-1673386
Pathogenesis of ANCA-Associated Pulmonary Vasculitis
Abstract
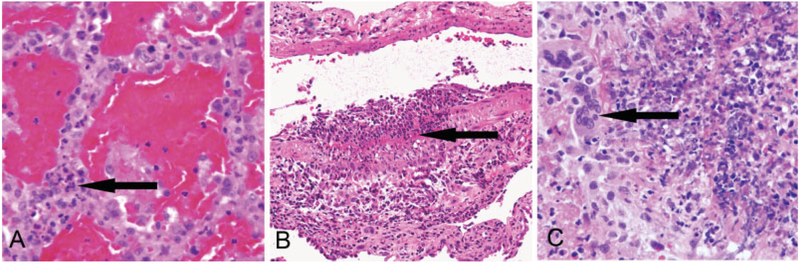
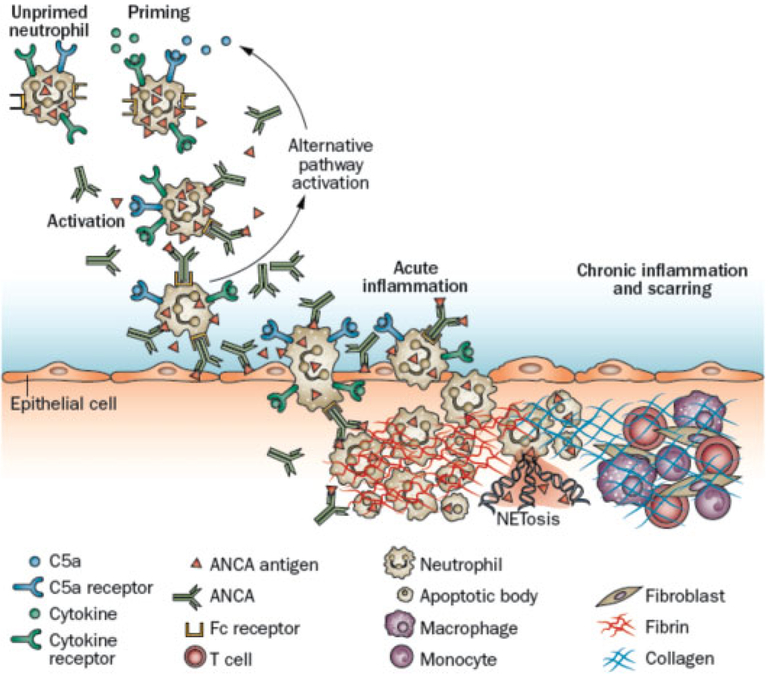
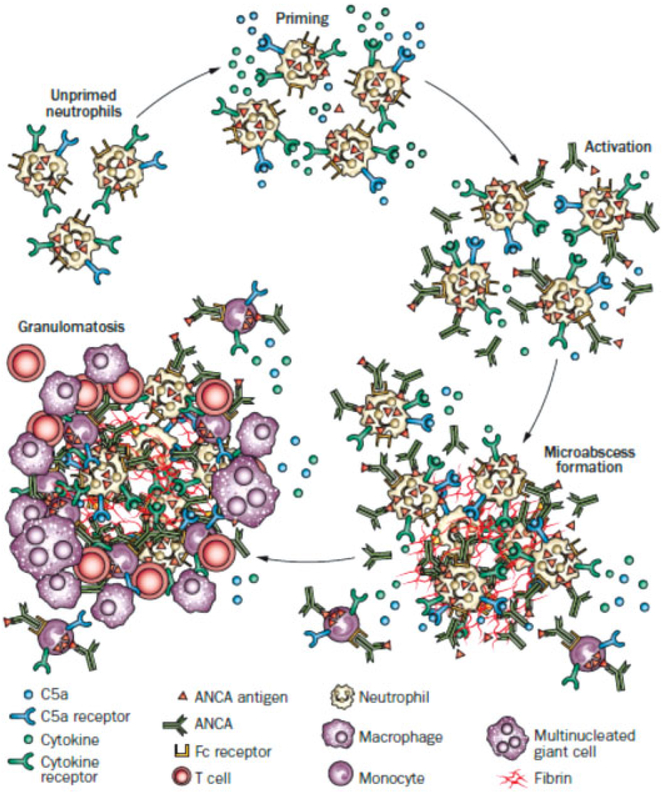
Antineutrophil cytoplasmic antibodies (ANCAs) are autoantibodies specific for antigens located in the cytoplasmic granules of neutrophils and lysosomes of monocytes. ANCAs are associated with a spectrum of necrotizing vasculitis that includes granulomatosis with polyangiitis, microscopic polyangiitis, and eosinophilic granulomatosis with polyangiitis. Pulmonary vasculitis and related extravascular inflammation and fibrosis are frequent components of ANCA vasculitis. In this review, we detail the factors that have been associated with the origin of the ANCA autoimmune response and summarize the most relevant clinical observations, in vitro evidence, and animal studies strongly indicating the pathogenic potential of ANCA. In addition, we describe the putative sequence of pathogenic mechanisms driven by ANCA-induced activation of neutrophils that result in small vessel necrotizing vasculitis and extravascular granulomatous necrotizing inflammation.
Thieme Medical Publishers 333 Seventh Avenue, New York, NY 10001, USA.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures

References
-
- Falk RJ, Jennette JC. Anti-neutrophil cytoplasmic autoantibodies with specificity for myeloperoxidase in patients with systemic vasculitis and idiopathic necrotizing and crescentic glomerulonephritis. N Engl J Med 1988;318(25):1651–1657 - PubMed
-
- Jennette JC, Falk RJ, Bacon PA, et al. 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum 2013;65(01):1–11 - PubMed
-
- Hoffman GS, Kerr GS, Leavitt RY,et al. Wegener granulomatosis: an analysis of 158 patients. Ann Intern Med 1992;116(06):488–498 - PubMed
-
- Anderson G, Coles ET, Crane M, et al. Wegener’s granuloma. A series of 265 British cases seen between 1975 and 1985. A report by a sub-committee of the British Thoracic Society Research Committee. QJ Med 1992;83(302):427–438 - PubMed
-
- Guillevin L, Durand-Gasselin B, Cevallos R, et al. Microscopic polyangiitis: clinical and laboratory findings in eighty-five patients. Arthritis Rheum 1999;42(03):421–430 - PubMed
