

A quest for sphincter-saving surgery in ultralow rectal tumours-a single-centre cohort study
- PMID: 30404633
- PMCID: PMC6223085
- DOI: 10.1186/s12957-018-1513-4
A quest for sphincter-saving surgery in ultralow rectal tumours-a single-centre cohort study
Abstract
Introduction: Despite the progress in the treatment of colorectal cancer, there is still no optimal strategy for tumours located adjacent to the anal sphincter. This study aims to evaluate oncological and functional results of surgery for rectal cancer in unfavourable locations in proximity to anal sphincters.
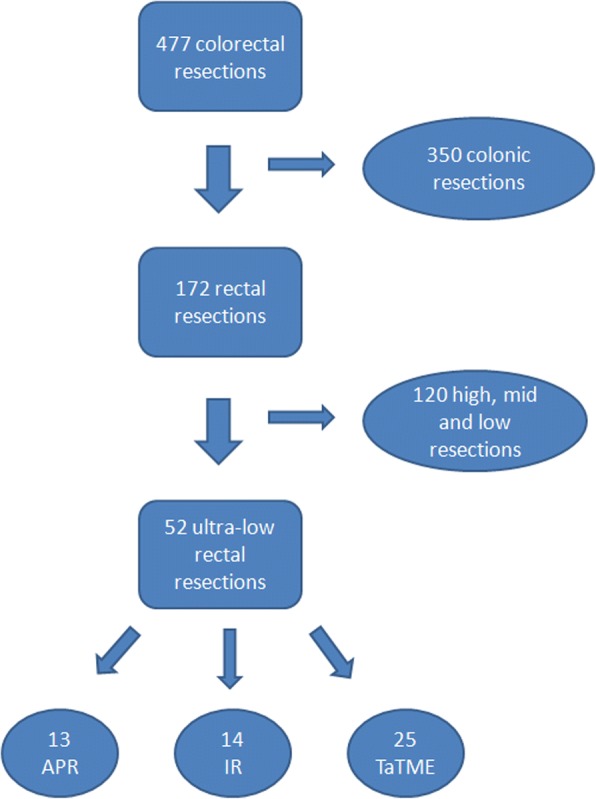
Materials and methods: Patients with rectal cancer, which was either initially infiltrating the anal sphincter or located in the close proximity of the sphincter, were included in the study. Patients were submitted to extralevator abdominoperineal resection (APR), intersphincteric resection, or transanal total mesorectal excision (TaTME). Primary outcomes were perioperative data: operative time, blood loss, complications, length of stay (LOS), and 30-day mortality. Secondary outcomes were pathological quality of the specimens and functional outcome 6 months after defunctioning ileostomy closure.
Results: Among patients with cancer adjacent to the anal sphincter, 13 (25%) underwent APR, 14 (27%) patients were submitted to intersphincteric resection, and 25 (48%) patients were treated with the TaTME approach. Operative time was 240 (210-270 IQR) for APR, 212.5 (170-260 IQR) for intersphincteric resection, and 270 (240-330 IQR) for TaTME (p = 0.018). Perioperative morbidity was 31% for APR, 36% for intersphincteric resections, and 12% for the TaTME group (p = 0.181). Complete mesorectal excision was achieved in 92% of specimens in the TaTME group, 93% in intersphincteric resections, and 78% in the APR group (p = 0.72). Median circumferential resection margin in APR was 6 mm (4-7 IQR), in intersphincteric resections 7.5 mm (2.5-10 IQR), and in the TaTME group 4 mm (2.8-8 IQR). All patients after intersphincteric resections developed major low anterior resection syndrome (LARS). Four patients in the TaTME group developed minor LARS, and 21 had major LARS.
Conclusion: Sphincter-saving rectal resections are a feasible alternative to APR with good clinical, pathological, and oncological outcomes. Intersphincteric resections and TaTME seem to be equal in terms of clinicopathological results. The functional outcome is yet to be investigated.
Trial registration: The study was retrospectively registered in Thai Clinical Trials Registry (23-07-2018, ID TCTR20180724001 ).
Keywords: Abdominoperineal resection; Intersphincteric resection; Rectal cancer; Transanal TME.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the Jagiellonian University Medical College Ethics Committee (No. 122.6120.198.2016).
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- How P, Shihab O, Tekkis P, Brown G, Quirke P, Heald R, Moran B. A systematic review of cancer related patient outcomes after anterior resection and abdominoperineal excision for rectal cancer in the total mesorectal excision era. Surg Oncol. 2011;20:e149–e155. doi: 10.1016/j.suronc.2011.05.001. - DOI - PubMed
-
- Okamura R, Hida K, Yamaguchi T, Akagi T, Konishi T, Yamamoto M, Ota M, Matoba S, Bando H, Goto S, Sakai Y, Watanabe M, Japan Society of Laparoscopic Colorectal Surgery. Watanabe K, Otsuka K, Takemasa I, Tanaka K, Ikeda M, Matsuda C, Fukuda M, Hasegawa J, Akamoto S, Shiozawa M, Tsuruta A, Akiyoshi T, Kato T, Tsukamoto S, Ito M, Naito M, Kanazawa A, Takahashi T, Ueki T, Hayashi Y, Morita S, Yamaguchi T, Nakanishi M, Hasegawa H, Okamoto K, Teraishi F, Sumi Y, Tashiro J, Yatsuoka T, Nishimura Y, Okita K, Kobatake T, Horie H, Miyakura Y, Ro H, Nagakari K, Hidaka E, Umemoto T, Nishigori H, Murata K, Wakayama F, Makizumi R, Fujii S, Sunami E, Kobayashi H, Nakagawa R, Enomoto T, Ohnuma S, Higashijima J, Ozawa H, Ashida K, Fujita F, Uehara K, Maruyama S, Ohyama M, Yamamoto S, Hinoi T, Yoshimitsu M, Okajima M, Tanimura S, Kawasaki M, Ide Y, Hazama S, Watanabe J, Inagaki D, Toyokawa A. Local control of sphincter-preserving procedures and abdominoperineal resection for locally advanced low rectal cancer: propensity score matched analysis. Ann Gastroenterol Surg. 2017;1:199–207. doi: 10.1002/ags3.12032. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
