

Obesity-associated Breast Inflammation among Hispanic/Latina Breast Cancer Patients
- PMID: 30404870
- PMCID: PMC6663483
- DOI: 10.1158/1940-6207.CAPR-18-0207
Obesity-associated Breast Inflammation among Hispanic/Latina Breast Cancer Patients
Abstract
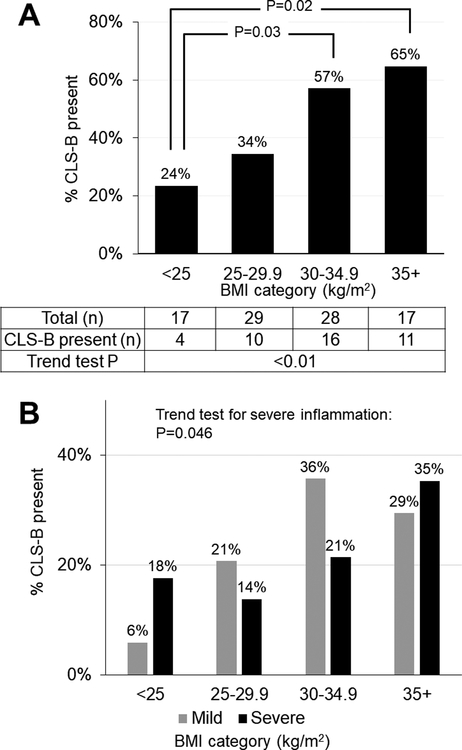
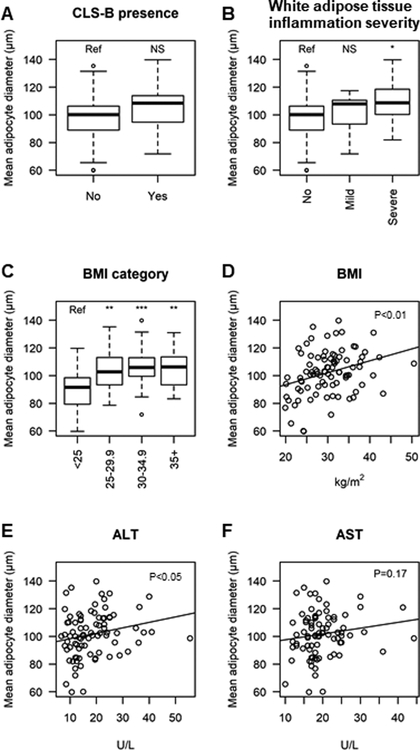
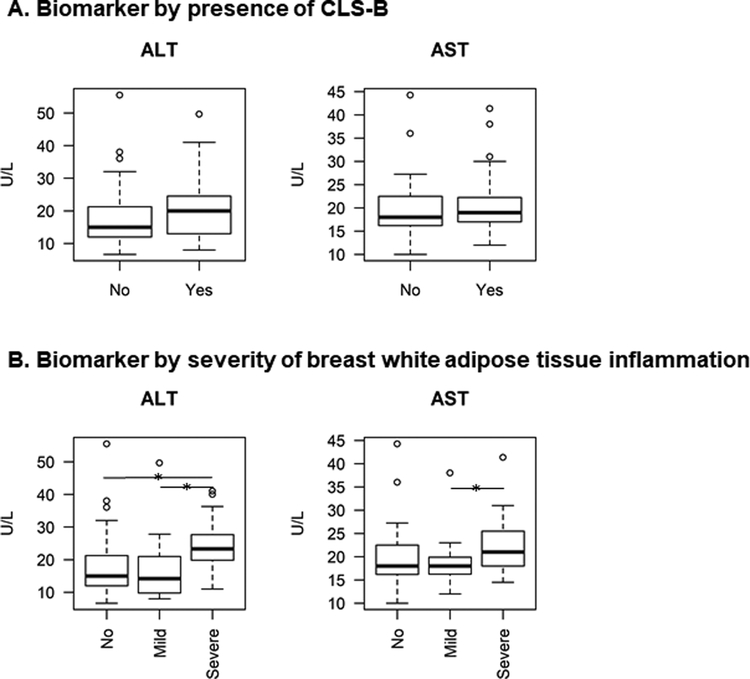
Breast white adipose tissue inflammation (BWATi) is associated with obesity and higher breast cancer risk among non-Hispanic white women. Obesity is prevalent in Hispanic/Latina patients with breast cancer, and the occurrence of BWATi in this population is not well-characterized. The association between BWATi and body mass index (BMI) was evaluated in Hispanic/Latina patients with breast cancer who underwent mastectomy. BWATi was defined as the presence of crown-like structures of the breast (CLS-B), detected by CD68 IHC in nontumor breast tissue. BWATi severity was quantified as number of CLS-B/cm2 Adipocyte diameter was measured using hematoxylin and eosin-stained breast tissue sections. Preoperative BMI (within 1 week prior to mastectomy) was categorized as normal (18.5-<25.0 kg/m2), overweight (25.0-<30.0 kg/m2), class I obesity (30.0-<35.0 kg/m2), and class II-III obesity (35.0 kg/m2 or above). Patient charts were abstracted to record clinicopathologic features and liver function tests <90 days before mastectomy. The study included 91 women (mean age 69 years; range 36-96 years). Prevalence of BWATi increased with BMI (24% in normal weight, 34% in overweight, 57% in class I obesity, and 65% in class II-III obesity; P trend <0.01). Severe BWATi (>0.27 CLS-B/cm2) was associated with higher BMI (P trend = 0.046) and greater adipocyte diameter (P = 0.04). Adjusting for BMI, neoadjuvant chemotherapy, and elevated alanine aminotransferase were associated with severe BWATi, and current smoking was associated with mild BWATi (all P < 0.05). BWATi was associated with higher BMI in Hispanic/Latina patients with breast cancer, consistent with previously described associations in other populations.
©2018 American Association for Cancer Research.
Conflict of interest statement
DISCLOSURE OF POTENTIAL CONFLICTS OF INTEREST
No potential conflicts of interest were disclosed.
Figures
References
-
- Morimoto LM, White E, Chen Z, Chlebowski RT, Hays J, Kuller L, et al. Obesity, body size, and risk of postmenopausal breast cancer: the Women’s Health Initiative (United States). Cancer Causes Control 2002;13(8):741–51. - PubMed
-
- Neuhouser ML, Aragaki AK, Prentice RL, Manson JE, Chlebowski R, Carty CL, et al. Overweight, Obesity, and Postmenopausal Invasive Breast Cancer Risk: A Secondary Analysis of the Women’s Health Initiative Randomized Clinical Trials. JAMA Oncol 2015;1(5):611–21 doi 10.1001/jamaoncol.2015.1546. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
