

Microbial Community Dynamics in Mother's Milk and Infant's Mouth and Gut in Moderately Preterm Infants
- PMID: 30405571
- PMCID: PMC6204356
- DOI: 10.3389/fmicb.2018.02512
Microbial Community Dynamics in Mother's Milk and Infant's Mouth and Gut in Moderately Preterm Infants
Abstract
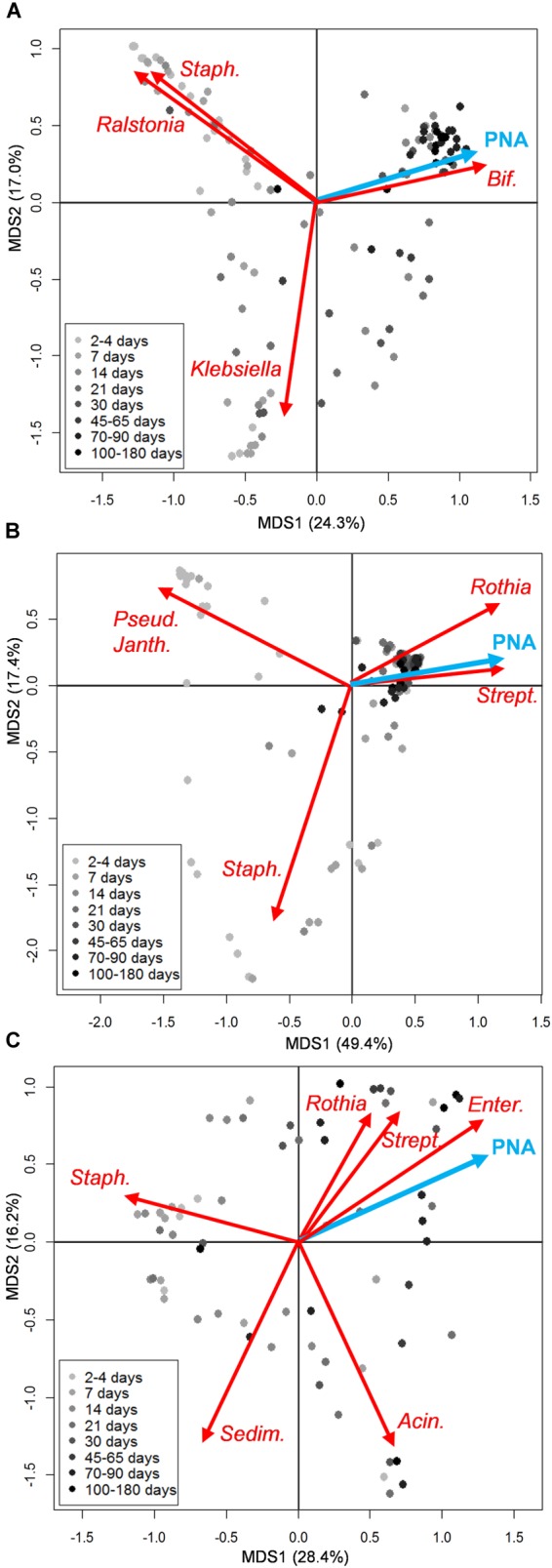
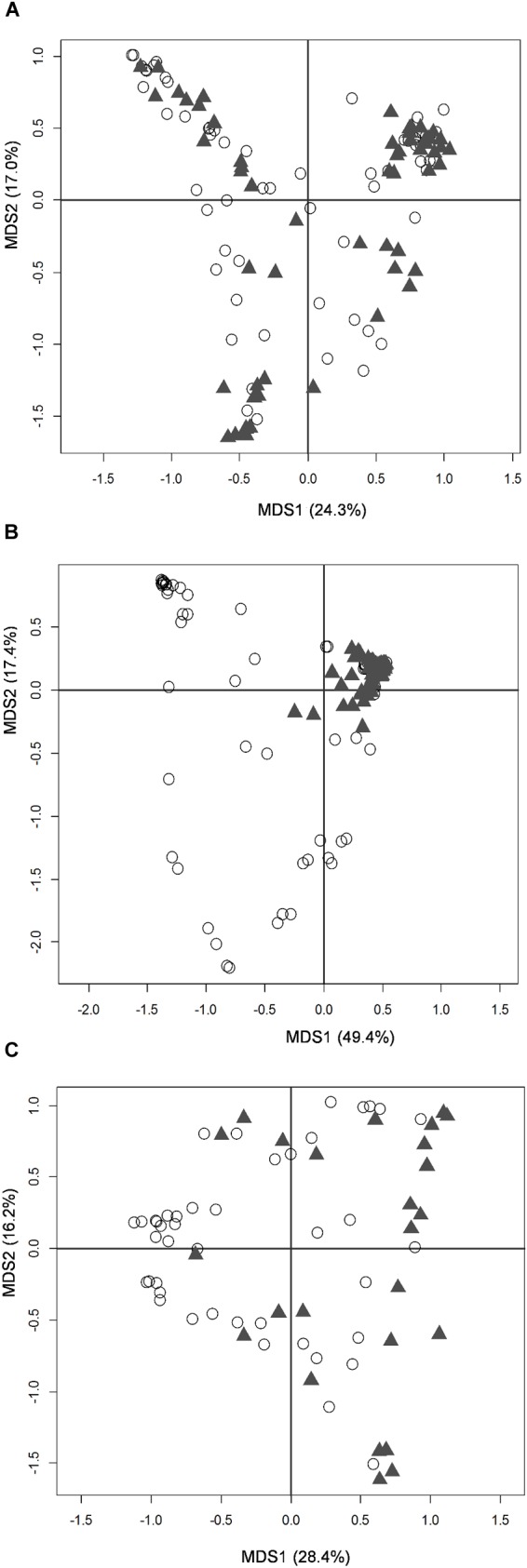
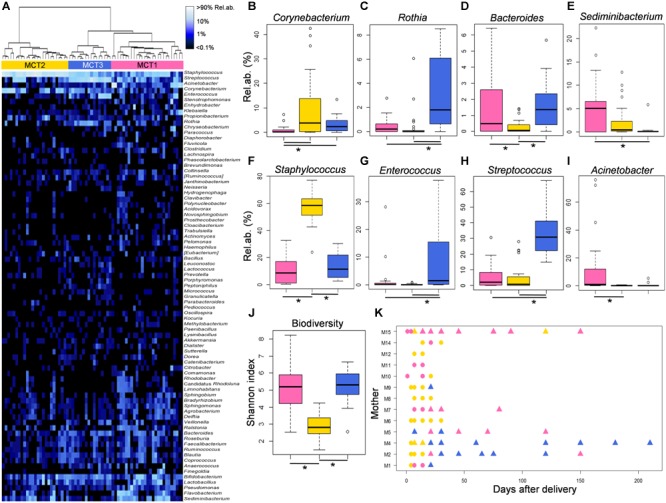
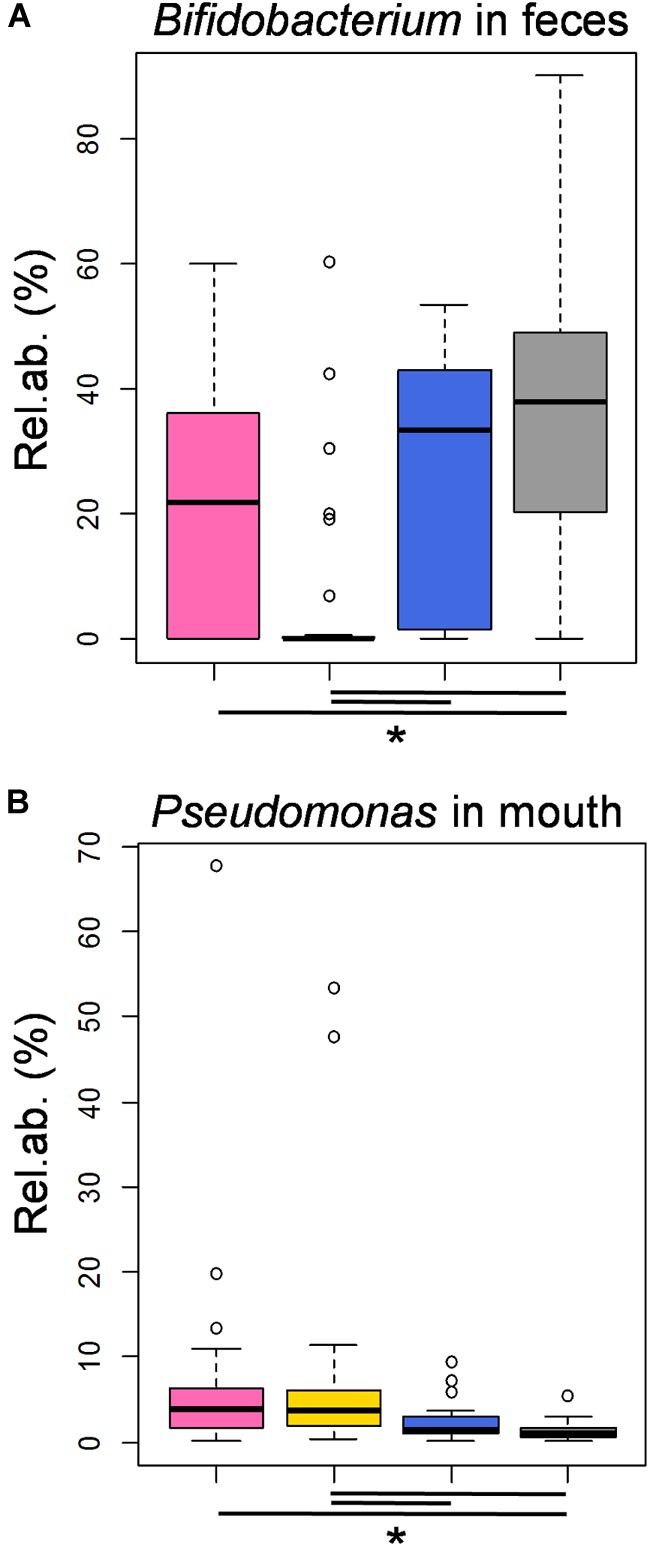
Mother's own milk represents the optimal source for preterm infant nutrition, as it promotes immune defenses and gastrointestinal function, protects against necrotizing enterocolitis, improves long-term clinical outcome and is hypothesized to drive gut microbiota assembly. Preterm infants at birth usually do not receive their mother's milk directly from the breast, because active suckling and coordination between suckling, swallowing and breathing do not develop until 32-34 weeks gestational age, but actual breastfeeding is usually possible as they grow older. Here, we enrolled moderately preterm infants (gestational age 32-34 weeks) to longitudinally characterize mothers' milk and infants' gut and oral microbiomes, up to more than 200 days after birth, through 16S rRNA sequencing. This peculiar population offers the chance to disentangle the differential contribution of human milk feeding per se vs. actual breastfeeding in the development of infant microbiomes, that have both been acknowledged as crucial contributors to short and long-term infant health status. In this cohort, the milk microbiome composition seemed to change following the infant's latching to the mother's breast, shifting toward a more diverse microbial community dominated by typical oral microbes, i.e., Streptococcus and Rothia. Even if all infants in the present study were fed human milk, features typical of healthy, full term, exclusively breastfed infants, i.e., high percentages of Bifidobacterium and low abundances of Pseudomonas in fecal and oral samples, respectively, were detected in samples taken after actual breastfeeding started. These findings underline the importance of encouraging not only human milk feeding, but also an early start of actual breastfeeding in preterm infants, since the infant's latching to the mother's breast might constitute an independent factor helping the health-promoting assembly of the infant gut microbiome.
Keywords: breastfeeding; infant gut microbiota; infant oral microbiota; latching; microbiota assembly; milk microbiota; moderately preterm infants.
Figures
References
LinkOut - more resources
Full Text Sources