

An Adaptive Seismocardiography (SCG)-ECG Multimodal Framework for Cardiac Gating Using Artificial Neural Networks
- PMID: 30405976
- PMCID: PMC6204924
- DOI: 10.1109/JTEHM.2018.2869141
An Adaptive Seismocardiography (SCG)-ECG Multimodal Framework for Cardiac Gating Using Artificial Neural Networks
Abstract
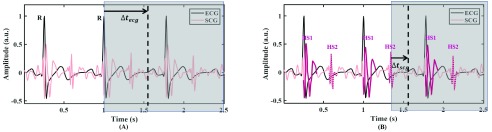
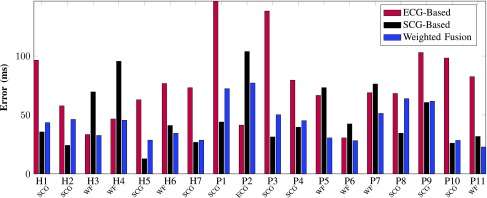
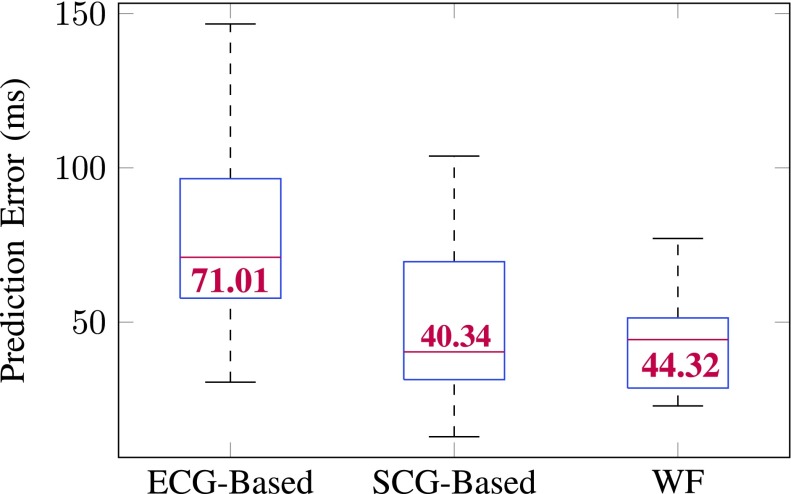
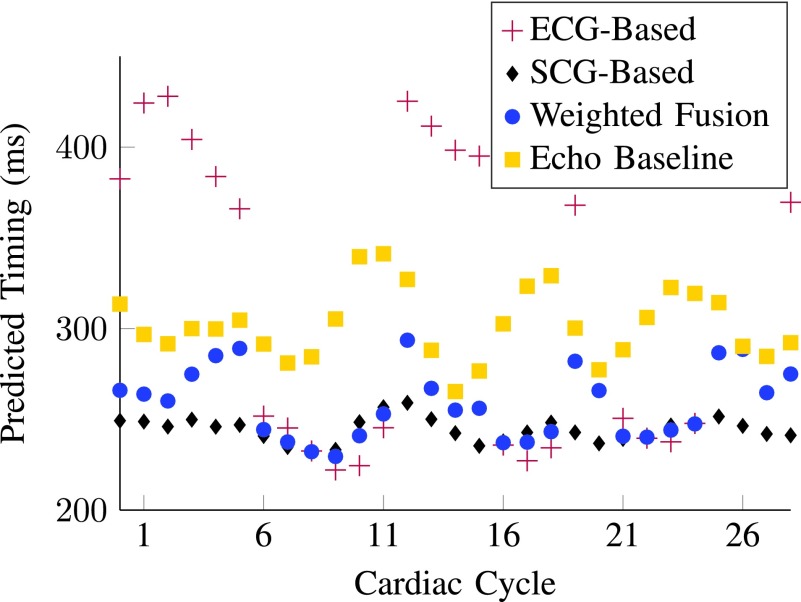
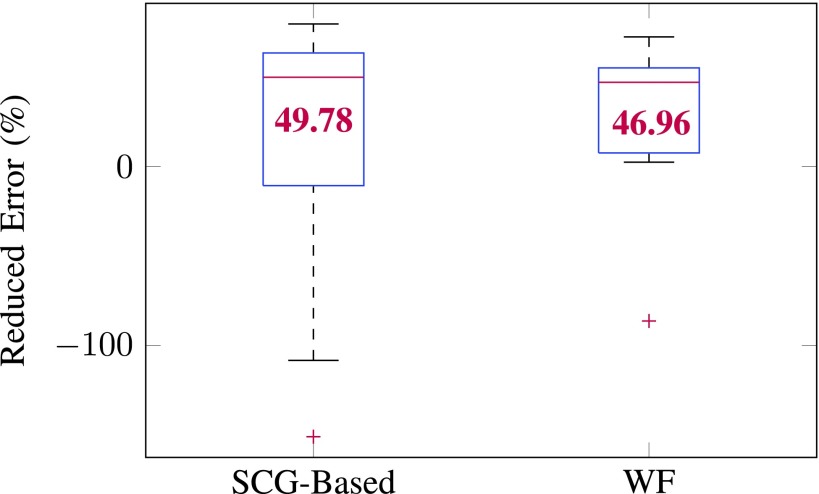
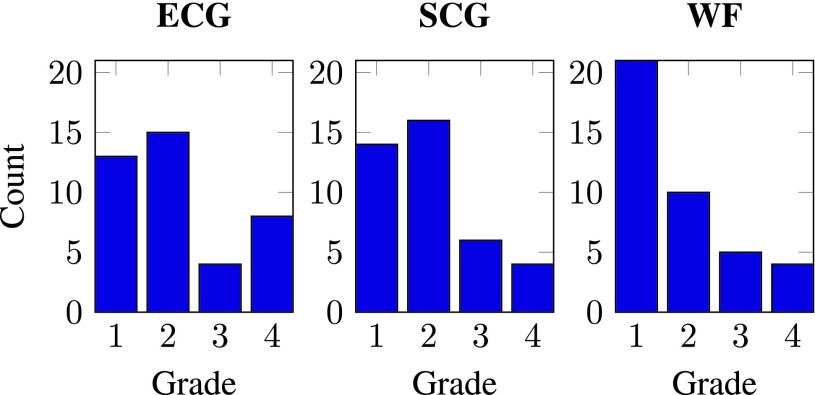
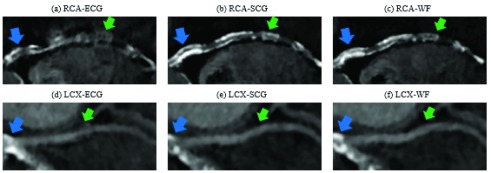
To more accurately trigger data acquisition and reduce radiation exposure of coronary computed tomography angiography (CCTA), a multimodal framework utilizing both electrocardiography (ECG) and seismocardiography (SCG) for CCTA prospective gating is presented. Relying upon a three-layer artificial neural network that adaptively fuses individual ECG- and SCG-based quiescence predictions on a beat-by-beat basis, this framework yields a personalized quiescence prediction for each cardiac cycle. This framework was tested on seven healthy subjects (age: 22-48; m/f: 4/3) and eleven cardiac patients (age: 31-78; m/f: 6/5). Seventeen out of 18 benefited from the fusion-based prediction as compared to the ECG-only-based prediction, the traditional prospective gating method. Only one patient whose SCG was compromised by noise was more suitable for ECG-only-based prediction. On average, our fused ECG-SCG-based method improves cardiac quiescence prediction by 47% over ECG-only-based method; with both compared against the gold standard, B-mode echocardiography. Fusion-based prediction is also more resistant to heart rate variability than ECG-only- or SCG-only-based prediction. To assess the clinical value, the diagnostic quality of the CCTA reconstructed volumes from the quiescence derived from ECG-, SCG- and fusion-based predictions were graded by a board-certified radiologist using a Likert response format. Grading results indicated the fusion-based prediction improved diagnostic quality. ECG may be a sub-optimal modality for quiescence prediction and can be enhanced by the multimodal framework. The combination of ECG and SCG signals for quiescence prediction bears promise for a more personalized and reliable approach than ECG-only-based method to predict cardiac quiescence for prospective CCTA gating.
Keywords: Artificial neural networks; cardiac gating; cardiac quiescence; computed tomography angiography; coronary angiography; echocardiography; electrocardiography; multimodal gating; seismocardiography.
Figures

References
-
- World Health Organization. (2017). Cardiovascular Disease. [Online]. Available: http://www.who.int/mediacentre/factsheets/fs317/en/
-
- Ricciardi M. J., Beohar N., and Davidson C. J., “Cardiac catheterization and coronary angiography,” in Essential Cardiology. Totowa, NJ, USA: Human Press, 2005, pp. 197–219.
-
- Desjardins B. and Kazerooni E. A., “ECG-gated cardiac CT,” Amer. J. Roentgenol., vol. 182, no. 4, pp. 993–1010, Apr. 2004. - PubMed
-
- Priest V. L., Scuffham P. A., Hachamovitch R., and Marwick T. H., “Cost-effectiveness of coronary computed tomography and cardiac stress imaging in the emergency department: A decision analytic model comparing diagnostic strategies for chest pain in patients at low risk of acute coronary syndromes,” Cardiovascular Imag., vol. 4, no. 5, pp. 549–556, 2011. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
