

A Case of Paraneoplastic Guillain-Barré Syndrome Associated with Squamous Cell Carcinoma of the Lung
- PMID: 30405981
- PMCID: PMC6205880
- DOI: 10.7759/cureus.3202
A Case of Paraneoplastic Guillain-Barré Syndrome Associated with Squamous Cell Carcinoma of the Lung
Abstract
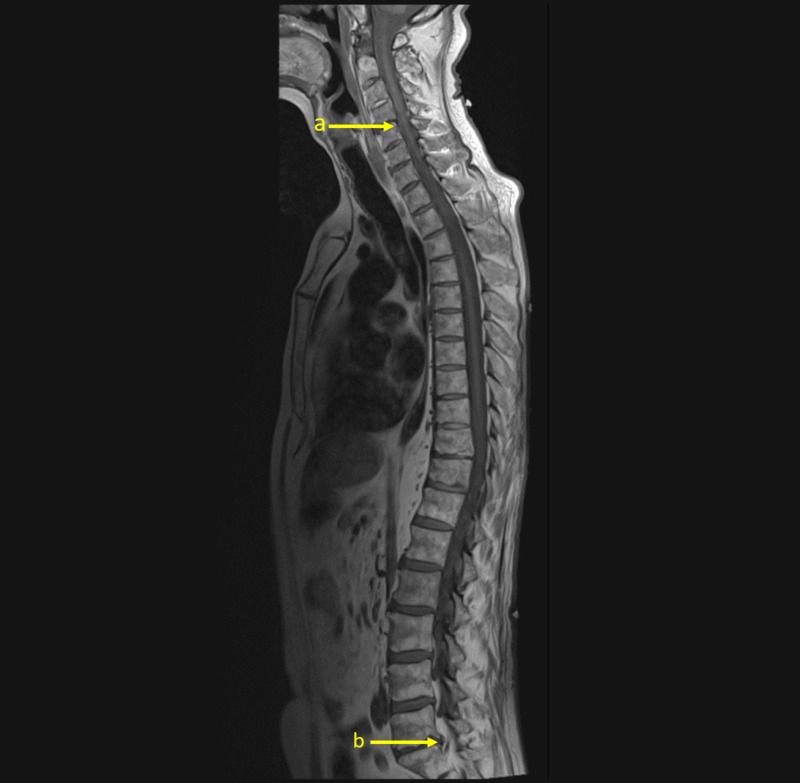
We report a case of a 61-year-old man with a history of squamous cell carcinoma of the lung presenting with rapidly progressive symmetric ascending weakness with areflexia. The weakness was quickly followed by respiratory decompensation requiring intubation. Lumbar puncture yielded cerebrospinal fluid with elevated protein (177 mg/dL), normal glucose (61 mg/dL), normal red blood cell count (0 per/µl), and normal white blood cell count (0 per/µL). Emergent magnetic resonance imaging of cervical, thoracic, and lumbar spine did not show evidence of metastatic disease, fracture, subluxation, or other causes of cord compression. The patient was diagnosed with acute inflammatory polyneuropathy, also known as Guillain-Barré syndrome. Despite treatment with a five-day course of intravenous immunoglobulin and a subsequent five-day course of plasmapheresis, the patient did not recover respiratory function and died 48 days after diagnosis. To our knowledge, this is the first documented case of Guillain-Barré occurring concomitantly with squamous cell carcinoma of the lung.
Keywords: guillain-barré syndrome; lung cancer; paraneoplastic; squamous cell cancer.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Guillain-Barré Syndrome After Acute Hepatitis E Infection: A Case Report and Literature Review.Crit Care Nurse. 2021 Aug 1;41(4):47-53. doi: 10.4037/ccn2021129. Crit Care Nurse. 2021. PMID: 34333618 Review.
-
Guillain-Barré syndrome in a patient with renal cell carcinoma following the first course of pazopanib therapy.J Infect Chemother. 2017 Nov;23(11):798-799. doi: 10.1016/j.jiac.2017.04.014. Epub 2017 May 13. J Infect Chemother. 2017. PMID: 28506529
-
An unusual case of recurrent Guillain-Barré syndrome with normal cerebrospinal fluid protein levels: a case report.BMC Neurol. 2016 Sep 5;16(1):161. doi: 10.1186/s12883-016-0687-z. BMC Neurol. 2016. PMID: 27596231 Free PMC article.
-
Guillain-Barré syndrome following thoracic spinal cord trauma.Can J Anaesth. 2008 Jul;55(7):441-6. doi: 10.1007/BF03016311. Can J Anaesth. 2008. PMID: 18591702
-
Guillain-Barré syndrome in children.Curr Opin Pediatr. 1995 Dec;7(6):663-8. doi: 10.1097/00008480-199512000-00006. Curr Opin Pediatr. 1995. PMID: 8776016 Review.
Cited by
-
Acute sensorimotor paraneoplastic neuropathy in a patient with small cell prostate cancer.BMJ Case Rep. 2024 Feb 27;17(2):e258380. doi: 10.1136/bcr-2023-258380. BMJ Case Rep. 2024. PMID: 38417933
-
Immunoglobulin unresponsive Guillain-Barré syndrome: rinse or repeat? A systematic review.BMJ Neurol Open. 2025 Feb 12;7(1):e000907. doi: 10.1136/bmjno-2024-000907. eCollection 2025. BMJ Neurol Open. 2025. PMID: 39950094 Free PMC article.
-
Cancer Diagnosis and Prognosis After Guillain-Barré Syndrome: A Population-Based Cohort Study.Clin Epidemiol. 2022 Jul 19;14:871-878. doi: 10.2147/CLEP.S369908. eCollection 2022. Clin Epidemiol. 2022. PMID: 35898330 Free PMC article.
References
-
- Guillain-Barré syndrome. Hughes RAC, Cornblath DR. Lancet. 2005;366:1653–1666. - PubMed
-
- Paraneoplastic syndromes involving the nervous system. Darnell RB, Posner JB. N Engl J Med. 2003;349:1543–1554. - PubMed
-
- Acute motor and sensory neuropathy associated with small-cell lung cancer: a clinicopathological study. Nokura K, Nagamatsu M, Inagaki T, et al. Neuropathology. 2006;26:329–337. - PubMed
-
- A case of Guillain-Barré syndrome in a patient with non small cell lung cancer treated with chemotherapy. Cicero G, Fulfaro F, Caraceni A, Arcara C, Badalamenti G, Intrivici C, Gebbia N. J Chemother. 2006;18:325–327. - PubMed
-
- Guillain-Barré-like syndrome heralding small-cell lung cancer. Eimil M, Benito-Leon J. Eur J Neurol. 2007;14:15–16. - PubMed
Publication types
LinkOut - more resources
Full Text Sources