

A Precision Medicine Approach to Cerebral Edema and Intracranial Hypertension after Severe Traumatic Brain Injury: Quo Vadis?
- PMID: 30406315
- PMCID: PMC6589108
- DOI: 10.1007/s11910-018-0912-9
A Precision Medicine Approach to Cerebral Edema and Intracranial Hypertension after Severe Traumatic Brain Injury: Quo Vadis?
Abstract
Purpose of review: Standard clinical protocols for treating cerebral edema and intracranial hypertension after severe TBI have remained remarkably similar over decades. Cerebral edema and intracranial hypertension are treated interchangeably when in fact intracranial pressure (ICP) is a proxy for cerebral edema but also other processes such as extent of mass lesions, hydrocephalus, or cerebral blood volume. A complex interplay of multiple molecular mechanisms results in cerebral edema after severe TBI, and these are not measured or targeted by current clinically available tools. Addressing these underpinnings may be key to preventing or treating cerebral edema and improving outcome after severe TBI.
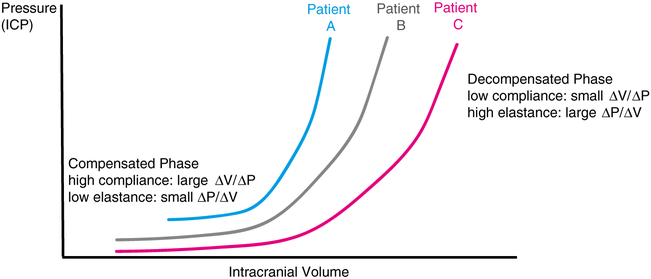
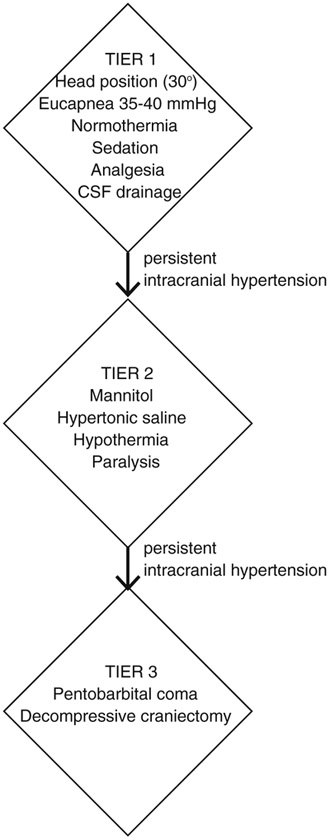
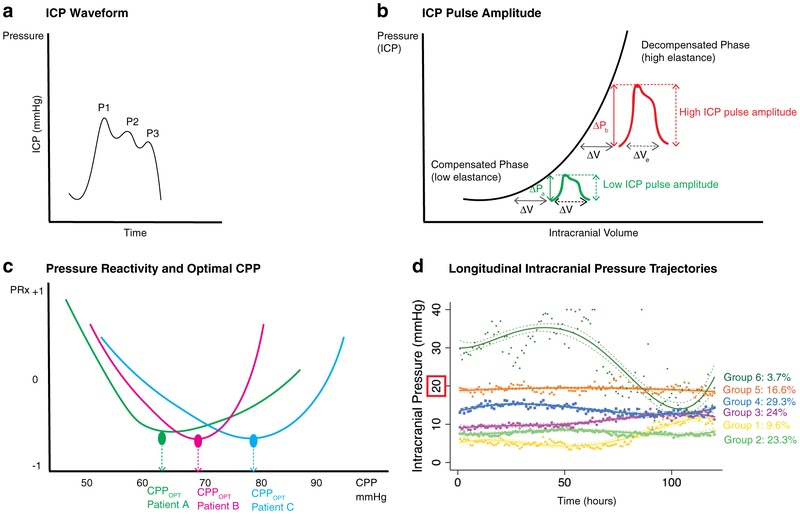
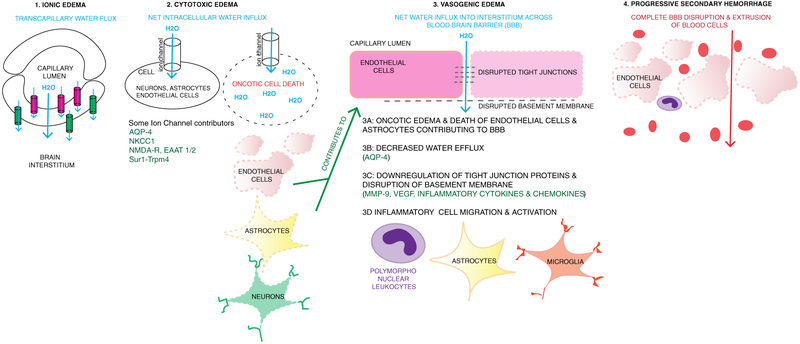
Recent findings: This review begins by outlining basic principles underlying the relationship between edema and ICP including the Monro-Kellie doctrine and concepts of intracranial compliance/elastance. There is a subsequent brief discussion of current guidelines for ICP monitoring/management. We then focus most of the review on an evolving precision medicine approach towards cerebral edema and intracranial hypertension after TBI. Personalization of invasive neuromonitoring parameters including ICP waveform analysis, pulse amplitude, pressure reactivity, and longitudinal trajectories are presented. This is followed by a discussion of cerebral edema subtypes (continuum of ionic/cytotoxic/vasogenic edema and progressive secondary hemorrhage). Mechanisms of potential molecular contributors to cerebral edema after TBI are reviewed. For each target, we present findings from preclinical models, and evaluate their clinical utility as biomarkers and therapeutic targets for cerebral edema reduction. This selection represents promising candidates with evidence from different research groups, overlap/inter-relatedness with other pathways, and clinical/translational potential. We outline an evolving precision medicine and translational approach towards cerebral edema and intracranial hypertension after severe TBI.
Keywords: Biomarkers; Cerebral edema; Intracranial hypertension; Severe traumatic brain injury; Therapeutic target.
Conflict of interest statement
Figures
References
-
-
Stocchetti N, Carbonara M, Citerio G, Ercole A, Skrifvars MB, Smielewski P, et al. Severe traumatic brain injury: targeted management in the intensive care unit. Lancet Neurol. 2017;16:452–64
Current review on management of severe TBI in the intensive care unit.
-
-
- Stocchetti N, Maas AIR. Traumatic intracranial hypertension. N Engl J Med. 2014;370:2121–30. - PubMed
-
- Winkler EA, Minter D, Yue JK, Manley GT. Cerebral edema in traumatic brain injury: pathophysiology and prospective therapeutic targets. Neurosurg Clin N Am. 2016;27:473–88. - PubMed
-
- Katayama Y, Mori T, Maeda T, Kawamata T. Pathogenesis of the mass effect of cerebral contusions: rapid increase in osmolality within the contusion necrosis. Acta Neurochir Suppl. 1998;71: 289–92. - PubMed
-
- Katayama Y, Kawamata T. Edema fluid accumulation within necrotic brain tissue as a cause of the mass effect of cerebral contusion in head trauma patients. Acta Neurochir Suppl (Wien). 2003;86:323–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
