

A Systematic Review on the Effect of HIV Infection on the Pharmacokinetics of First-Line Tuberculosis Drugs
- PMID: 30406475
- PMCID: PMC7019645
- DOI: 10.1007/s40262-018-0716-8
A Systematic Review on the Effect of HIV Infection on the Pharmacokinetics of First-Line Tuberculosis Drugs
Abstract
Introduction: Contrasting findings have been published regarding the effect of human immunodeficiency virus (HIV) on tuberculosis (TB) drug pharmacokinetics (PK).
Objectives: The aim of this systematic review was to investigate the effect of HIV infection on the PK of the first-line TB drugs (FLDs) rifampicin, isoniazid, pyrazinamide and ethambutol by assessing all published literature.
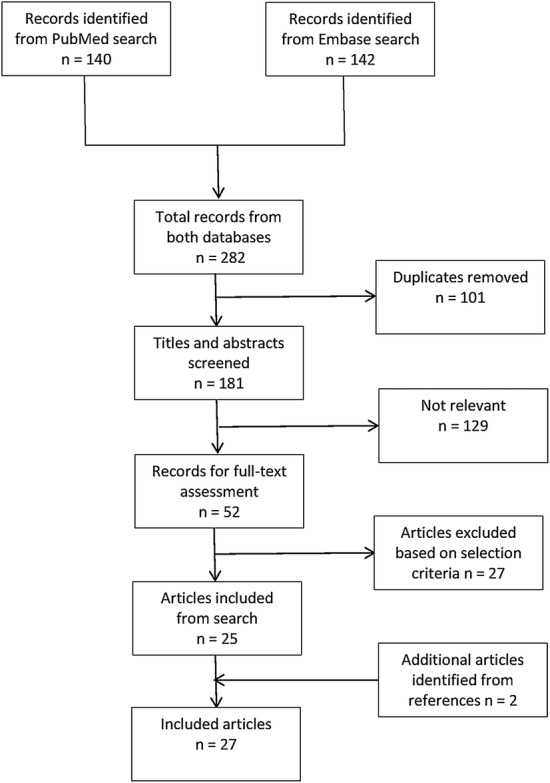
Methods: Searches were performed in MEDLINE (through PubMed) and EMBASE to find original studies evaluating the effect of HIV infection on the PK of FLDs. The included studies were assessed for bias and clinical relevance. PK data were extracted to provide insight into the difference of FLD PK between HIV-positive and HIV-negative TB patients. This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement and its protocol was registered at PROSPERO (registration number CRD42017067250).
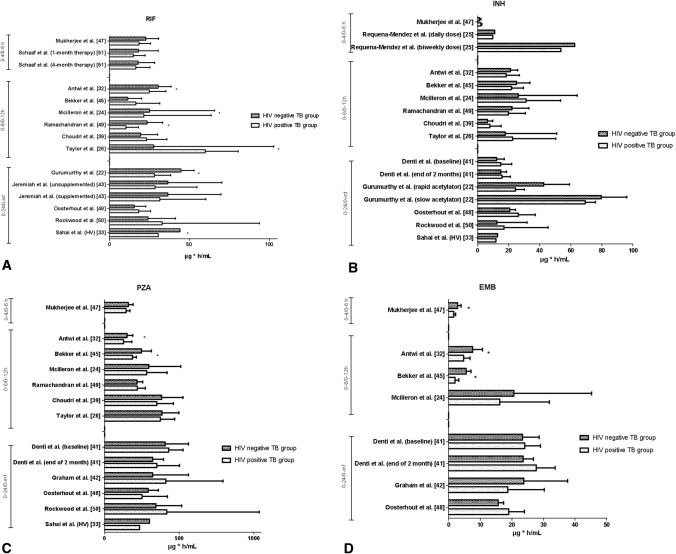
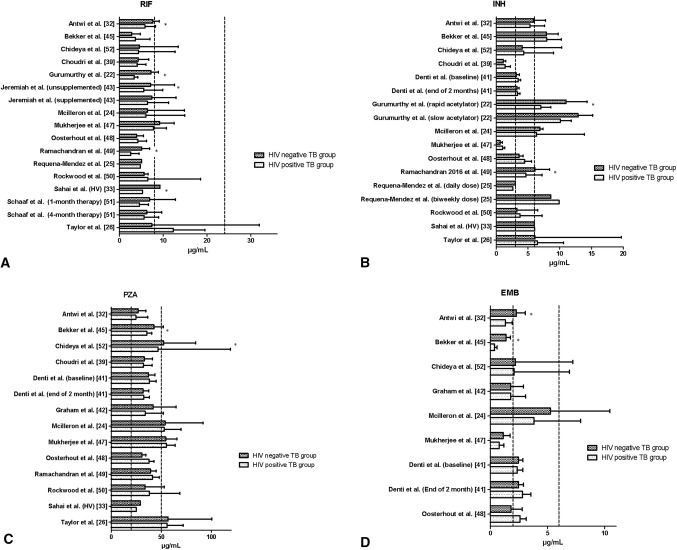
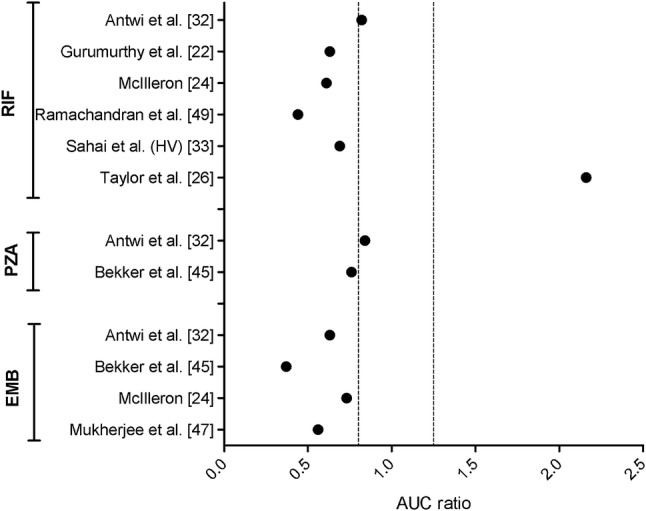
Results: Overall, 27 studies were eligible for inclusion. The available studies provide a heterogeneous dataset from which consistent results could not be obtained. In both HIV-positive and HIV-negative TB groups, rifampicin (13 of 15) and ethambutol (4 of 8) peak concentration (Cmax) often did not achieve the minimum reference values. More than half of the studies (11 of 20) that included both HIV-positive and HIV-negative TB groups showed statistically significantly altered FLD area under the concentration-time curve and/or Cmax for at least one FLD.
Conclusions: HIV infection may be one of several factors that reduce FLD exposure. We could not make general recommendations with respect to the role of dosing. There is a need for consistent and homogeneous studies to be conducted.
Conflict of interest statement
Alper Daskapan, Lusiana R. Idrus, Maarten J. Postma, Bob Wilffert, Jos G. W. Kosterink, Ymkje Stienstra, Daniel J. Touw, Aase B. Andersen, Adrie Bekker, Paolo Denti, Agibothu K. Hemanth Kumar, Kidola Jeremiah, Awewura Kwara, Helen McIlleron, Graeme Meintjes, Joep J. van Oosterhout, Geetha Ramachandran, Neesha Rockwood, Robert J. Wilkinson, Tjip S. van der Werf and Jan-Willem C. Alffenaar declare that they have no conflicts of interest.
Figures
References
-
- World Health Organization. Global tuberculosis report 2016; 2016. http://www.who.int/tb/publications/global_report/en/. Accessed 25 June 2017.
-
- UNAIDS. Global AIDS update 2016; 2016. http://www.unaids.org/en/resources/documents/2016/Global-AIDS-update-2016. Accessed 25 June 2017.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
