

Rutosides for treatment of post-thrombotic syndrome
- PMID: 30406640
- PMCID: PMC6517027
- DOI: 10.1002/14651858.CD005625.pub4
Rutosides for treatment of post-thrombotic syndrome
Abstract
Background: Post-thrombotic syndrome (PTS) is a long-term complication of deep venous thrombosis (DVT) that is characterised by pain, swelling, and skin changes in the affected limb. One in three patients with DVT will develop post-thrombotic sequelae within five years. Rutosides are a group of compounds derived from horse chestnut (Aesculus hippocastanum), a traditional herbal remedy for treating oedema formation in chronic venous insufficiency (CVI). However, it is not known whether rutosides are effective and safe in the treatment of PTS. This is the second update of the review first published in 2013.
Objectives: To determine the effectiveness (improvement or deterioration in symptoms) and safety of rutosides for treatment of post-thrombotic syndrome (PTS) in patients with DVT compared to placebo, no intervention, elastic compression stockings (ECS) or any other treatment.
Search methods: The Cochrane Vascular Information Specialist searched the Cochrane Vascular Specialised Register, CENTRAL, MEDLINE, Embase and CINAHL databases and World Health Organization International Clinical Trials Registry Platform and ClinicalTrials.gov trials registers to 21 August 2018.
Selection criteria: Two review authors independently assessed studies for inclusion. Studies were included to allow the comparison of rutosides versus placebo or no treatment, rutosides versus ECS, and rutosides versus any other treatment. Two review authors extracted information from the trials. Disagreements were resolved by discussion.
Data collection and analysis: Data were extracted using designated data extraction forms. The Cochrane 'Risk of bias' tool was used for all included studies to assist in the assessment of quality. Primary outcome measures were the occurrence of leg ulceration over time (yes or no) and any improvement or deterioration of post-thrombotic syndrome (yes or no). Secondary outcomes included reduction of oedema, pain, recurrence of DVT or pulmonary embolism, compliance with therapy, and adverse effects. All of the outcome measures were analysed using Mantel-Haenzel fixed-effect model odds ratios. The unit of analysis was the number of patients. We used GRADE to assess the quality of the evidence for each outcome.
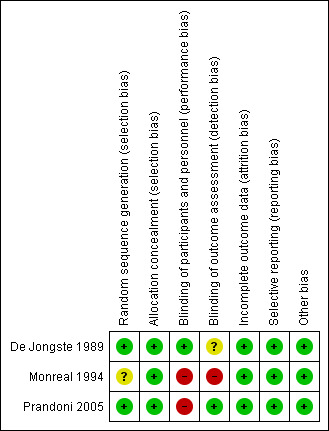
Main results: Ten reports of nine studies were identified following searching and three studies with a total of 233 participants met the inclusion criteria. Overall quality of evidence using the GRADE approach was low, predominantly due to the lack of both participant and researcher blinding in the included studies. The quality of the evidence was further limited as only three small studies contributed to the review findings. A subjective scoring system was used to obtain the symptoms of PTS so it was important that the assessors were blinded to the intervention. One study compared rutosides with placebo, one study compared rutosides with ECS and rutosides plus ECS versus ECS alone, and one study compared rutosides with an alternative venoactive remedy. Occurrence of leg ulceration was not reported in any of the included studies. There was no clear evidence to support a difference in PTS improvement between the rutosides or placebo/no treatment groups (OR 1.29, 95% CI 0.69 to 2.41; 164 participants; 2 studies; low-quality evidence); or between the rutosides and ECS groups (OR 0.80, 95% CI 0.31 to 2.03; 80 participants; 1 study ; low-quality evidence). Results from one small study reported less PTS improvement in the rutosides group compared to an alternative venoactive remedy (OR 0.18, 95% CI 0.04 to 0.94; 29 participants; 1 study; low-quality evidence). There was no clear evidence to support a difference in PTS deterioration when comparing rutosides with placebo/no treatment (OR 0.61, 95% CI 0.19 to 1.90; 80 participants; 1 study); with ECS (OR 0.61, 95% CI 0.19 to 1.90; 80 participants; 1 study); or an alternative venoactive remedy (OR 0.19, 95% CI 0.01 to 4.24; 29 participants; 1 study). No clear evidence of a difference in adverse effects between the rutosides and placebo/no treatment groups was seen ('mild side effects' reported in 7/41 and 5/42 respectively). In the study comparing rutosides with ECS, 2/80 could not tolerate ECS and 6/80 stopped medication due to side effects. The study comparing rutosides with an alternative venoactive remedy did not comment on side effects AUTHORS' CONCLUSIONS: There was no evidence that rutosides were superior to the use of placebo or ECS. Overall, there is currently limited low-quality evidence that 'venoactive' or 'phlebotonic' remedies such as rutosides reduce symptoms of PTS. Mild side effects were noted in one study. The three studies included in this review provide no evidence to support the use of rutosides in the treatment of PTS.
Conflict of interest statement
JM: declared that she is currently receiving a MRC Clinicial Scientist Fellowship grant which does not conflict with this review CB: works within the Cochrane Vascular editorial base. Where necessary, editorial tasks were carried out by other members of the group SEY: none known DK: none known
Figures













Update of
-
Rutosides for treatment of post-thrombotic syndrome.Cochrane Database Syst Rev. 2015 Sep 16;(9):CD005625. doi: 10.1002/14651858.CD005625.pub3. Cochrane Database Syst Rev. 2015. Update in: Cochrane Database Syst Rev. 2018 Nov 08;11:CD005625. doi: 10.1002/14651858.CD005625.pub4. PMID: 26376212 Updated.
References
References to studies included in this review
De Jongste 1989 {published data only}
-
- Jongste AB, Jonker JJ, Huisman MV, Cate JW, Azar AJ. A double blind three center clinical trial on the short‐term efficacy of 0‐(beta‐hydroxyethyl)‐rutosides in patients with post‐thrombotic syndrome. Thrombosis and Haemostasis 1989;62(3):826‐9. - PubMed
-
- Jongste AB, Jonker JJC, Huisman MV, Cate JW, Azar AJ. A double‐blind trial on the short‐term efficacy of HR in patients with the post‐thrombotic syndrome. Phlebology 1990;5 Suppl 1:21‐2.
Monreal 1994 {published data only}
-
- Monreal M, Callejas JM, Martorell A, Lisbona C, Lerma R. A prospective study of the long‐term efficacy of two different venoactive drugs in patients with post‐thrombotic syndrome. Phlebology 1994;9:37‐40.
Prandoni 2005 {published data only}
-
- Prandoni P. Elastic stockings, hydroxyethylrutosides or both for the treatment of post‐thrombotic syndrome. Thrombosis and Haemostasis 2005;93(1):183‐5. - PubMed
References to studies excluded from this review
Cospite 1986 {published data only}
-
- Cospite M, Amato C, Milio G, Scrivano V. Changes of venous haemodynamics in subjects with post‐thrombotic syndrome, treated with high doses of diosmine in association with other bioflavonoids. What is New in Angiology? Trends and Controversies. Zuckschwerdt W, 1986.
De Jongste 1986 {published data only}
-
- Jongste AB, Cate JW, Huisman MV. The effectiveness of 0‐(beta‐hydroxyethyl)‐rutosides (HR) in the post‐thrombotic syndrome (PTS). Phlebology'85. John Libbey and Co. Ltd, 1986:837‐9.
Diebschlag 1994 {published data only}
-
- Diebschlag W, Nocker W, Lehmacher W, Rehn D. A clinical comparison of two doses of 0‐(beta‐Hydroxyethyl)‐rutosides (oxerutins) in patients with chronic venous insufficiency. Journal of Pharmaceutical Medicine 1994;4(1):7‐14.
Incandela 2002 {published data only}
-
- Incandela L, Belcaro G, Renton S, DeSanctis MT, Cesarone MR, Bavera, et al. HR (Paroven, Venoruton; 0‐(beta‐hydroxyethyl)‐rutosides) in venous hypertensive microangiopathy: a prospective, placebo‐controlled, randomized trial. Journal of Cardiovascular Pharmacology and Therapeutics 2002;7 Suppl 1:S7‐10. - PubMed
Nill 1970 {published data only}
-
- Nill HJ, Fischer H. Comparative investigations concerning the effect of extract of horse chestnut upon the pressure‐volume‐diagram of patients with venous disorders [Vergleichende Untersuchungen zur Beeinflussung des Druck‐Volumen‐Diagramms durch Roßkastanienextrakt bei Venenkranken]. Arztliche Forschung 1970;24(5):141‐3. - PubMed
Rose 1970 {published data only}
-
- Rose SS. A report on the use of an hydroxyethylrutoside in symptoms due to venous back pressure and allied conditions in the lower limbs. British Journal of Clinical Practice 1970;24(4):161‐4. - PubMed
Additional references
Bombardelli 1996
-
- Bombardelli E, Morazzoni P, Griffini A. Aesculus hippocastanum L. Fitoterapia 1996;67(6):483‐511.
Cesarone 2005
-
- Cesarone MR, Belcaro G, Pellegrini L, Ledda A, Vinciguerra G, Ricci A, et al. HR, 0‐(beta‐hydroxyethyl)‐rutosides; (Venoruton): rapid relief of signs/symptoms in chronic venous insufficiency and microangiopathy: a prospective, controlled study. Angiology 2005;56(2):165‐72. - PubMed
Cohen 2012
-
- Cohen JM, Akl EA, Kahn SR. Pharmacologic and compression therapies for postthrombotic syndrome: a systematic review of randomized controlled trials. Chest 2012;141(2):308‐20. - PubMed
Facino 1995
-
- Facino RM, Carini M, Stefani R, Aldini G, Saibene L. Anti‐elastase and anti‐hyaluronidase activities of saponins and sapogenins from Hedera helix, Aesculus hippocastanum, and Ruscus aculeatus: factors contributing to their efficacy in the treatment of venous insufficiency. Archiv der Pharmazie 1995;328(10):720‐4. - PubMed
Guillaume 1994
-
- Guillaume M, Padioleau F. Veinotonic effect, vascular protection, antiinflammatory and free radical scavenging properties of horse chestnut extract. Arzneimittel‐Forschung 1994;44(1):25‐35. - PubMed
Higgins 2011
-
- Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available at handbook.cochrane.org.
Kahn 2009
-
- Kahn SR, Partsch H, Vedantham S, Prandoni P, Kearon C, Subcommittee on control of anticoagulation of the scientific and standardization committee of the International Society on Thrombosis and Haemostasis. Definition of post‐thrombotic syndrome of the leg for use in clinical investigations: a recommendation for standardization. Journal of Thrombosis and Haemostasis 2009;7(5):879‐83. - PubMed
Lefebvre 2011
-
- Lefebvre C, Manheimer E, Glanville J. Chapter 6: Searching for studies. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Lorenz 1960
-
- Lorenz D, Marek ML. Das therapeutische wirksame Prinzip der Rosskastanie (Aesculus hippocastanum). Arzneimittel‐Forschung/Drug Research 1960;10:263‐72. - PubMed
Morling 2018
Moyses 1987
-
- Moyses C, Cederholm‐Williams SA, Michel CC. Haemoconcentration and accumulation of white cells in the feet during venous stasis. International Journal of Microcirculation: Clinical and Experimental 1987;5(4):311‐20. - PubMed
Partsch 1991
-
- Partsch H. Compression therapy of the legs. A review. Journal of Dermatologic Surgery and Oncology 1991;17(10):799‐805. - PubMed
Pittler 2012
Prandoni 1996
-
- Prandoni P, Lensing AW, Cogo A, Cuppini S, Villalta S, Carta M, et al. The long‐term clinical course of acute deep venous thrombosis. Annals of Internal Medicine 1996;125(1):1‐7. - PubMed
Sarin 1993
-
- Sarin S, Andaz A, Shields DA, Scurr JH, Coleridge Smith PD. Neutrophil activation in venous disease. Journal of Vascular Surgery 1993;17:444.
Schrader 1995
-
- Schrader E, Schwankl W, Sieder C, Christoffel V. Comparison of the bioavailability of beta‐aescin after single oral administration of two different drug formulations containing an extract of horse‐chestnut seeds [Vergleichende Untersuchung zur Bioverfügbarkeit von ß‐Aescin nach oraler Einmalverabreichung zweier Rosskastaniensamenextrakt enthaltender, galenisch unterschiedlicher Darreichungsformen]. Pharmazie 1995;50(9):623‐7. - PubMed
Thomas 1988
Villalta 1994
-
- Villalta S, Bagatella P, Piccioli A, Lensing A, Prins M, Prandoni P. Assessment of validity and reproducibility of a clinical scale for the post‐thrombotic syndrome. Haemostasis 1994;24:158a.
References to other published versions of this review
Kolbach 2006
Morling 2013
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous