

Contemporary management of renal trauma in Canada: A 10-year experience at a level 1 trauma centre
- PMID: 30407154
- PMCID: PMC6570592
- DOI: 10.5489/cuaj.5581
Contemporary management of renal trauma in Canada: A 10-year experience at a level 1 trauma centre
Abstract
Introduction: Contemporary Canadian renal trauma data is lacking. Our objective is to describe 10-year outcomes of renal trauma at a Canadian level 1 trauma centre using a conservative approach.
Methods: The Alberta Trauma Registry at the University of Alberta was used to identify renal trauma patients from October 2004 to December 2014. Hospital records and imaging were reviewed to identify clinic-radiographical factors, including patient age, gender, Injury Severity Score (ISS), American Association of the Surgery for Trauma (AAST) grade, computerized tomography (CT) findings, urological interventions, length of stay, transfusion and death rates. Descriptive statistics, Chi-square, and t-tests were used when appropriate.
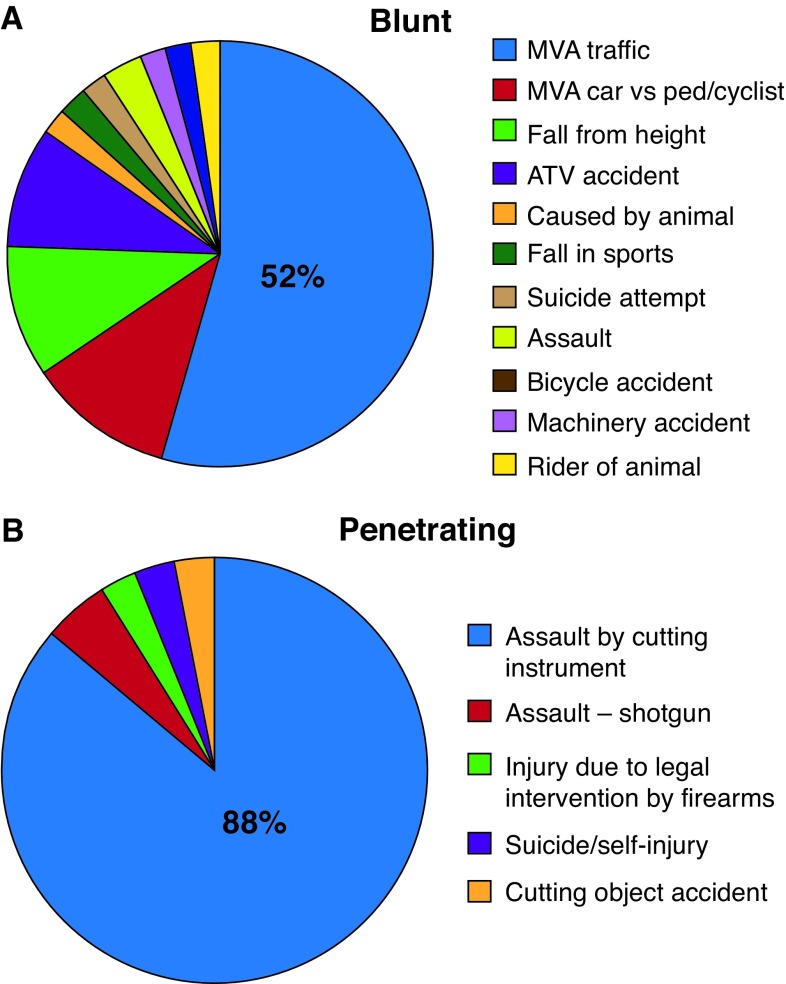
Results: A total of 368 renal trauma patients were identified. Mechanism of injury was blunt trauma in 89.1% of cases, mean age was 36.2 years, and mean ISS was 30.8 (±13.6). AAST grade distribution was 16.6% (Grade 1), 22.8% (Grade 2), 36.4% (Grade 3), 20.9% (Grade 4), and 3.3% (Grade 5). Overall, 9.5% (35) of patients required urological intervention for a total of 40 treatments, including ureteral stenting (3.0%), angioembolization (3.3%), percutaneous drainage (0.3%), or open intervention including nephrectomy (2.4%) and renorrhaphy (0.5%). No Grade 1 or 2 injuries required intervention, while 1.5%, 31.2%, and 75.0% of Grade 3, 4, and 5 injuries did, respectively. The overall renal salvage rate was 97.6%, which did not differ by mechanism of injury (p=0.25). Patients with penetrating trauma were more likely to require urological intervention (20.0% vs. 8.2%; p=0.04). Of the high-grade (III-V) renal injuries identified, 15.7% (35/223) required urological intervention, 4.9% (11) required open surgical intervention, and only 4.0% (9) of patients with high-grade renal injury required nephrectomy.
Conclusions: The trend towards conservative treatment of renal trauma in Canada appears well-supported even in a severely injured patient population, as over 90% of patients avoid urological intervention and only 3% require operative intervention resulting in renal salvage rates of 97.6%.
Conflict of interest statement
Figures
References
LinkOut - more resources
Full Text Sources
