

Novel presentations of periodic fever syndromes: Discrepancies between genetic and clinical diagnoses
- PMID: 30407166
- PMCID: PMC6459325
- DOI: 10.5152/eurjrheum.2018.18023
Novel presentations of periodic fever syndromes: Discrepancies between genetic and clinical diagnoses
Abstract
Objective: The Periodic fever syndromes (PFS) are a group of disorders of the innate immune system. We investigated patients diagnosed with PFS at the Dartmouth Hitchcock Pediatric Rheumatology Clinic.
Methods: Case acquisition was performed by reviewing ICD 9/10 coded records for familial Mediterranean fever (ICD 9 277.31), laboratory test records for PFS genetic screening, and clinic records between 1/1/2011 and 12/31/2017.
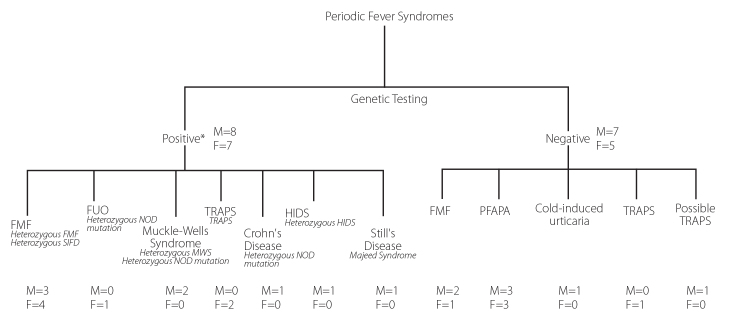
Results: Twenty-seven cases had clinical evaluations including PFS genetic screening. Clinical diagnoses included familial Mediterranean fever (FMF) (10 cases), Muckle-Wells (2 cases), tumor necrosis factor receptor associated periodic syndrome (TRAPS) (4 cases), hyper IgD syndrome (HIDS) (1 case), Crohn's Disease (1 case), systemic onset juvenile idiopathic arthritis (SoJIA) (1 case), fever of unknown origin (FUO) (1 case), periodic fever adenitis pharyngitis aphthous ulcer (PFAPA) (6 cases), and cold-induced urticaria (1 case). Fifteen cases were associated with a genetic cause. Seven of the 10 FMF cases were confirmed genetically and were either heterozygous or compound heterozygotes. Both cases of Muckle-Wells had either a compound heterozygote for CIAS 1 or a NOD gene mutation. Both TRAPS cases presented atypically with patients developing systemic lupus erythematosus (SLE) or being asymptomatic. Two patients had novel syndromes. One FMF patient had a TRNT1 gene mutation who responded to intravenous immunoglobulin (IVIg) and colchicine after failing multiple treatments. The other had SoJIA with a LPIN 2 gene mutation but responded to colchicine. Only one of the 15 genetically proven cases had classical presentation and genetics (HIDS secondary to a mevalonate kinase (MVK) gene mutation).
Conclusion: PFS screening was helpful in over half of the cases to develop therapeutic treatment plans. Given the atypical clinical presentations seen with genetically determined PFS, extensive genetic testing is indicated for all patients presenting with a PFS, excluding classical PFAPA syndrome.
Conflict of interest statement
Figures
References
-
- Durrant K, Ignacio Arostegui J. Comparison Chart of Systemic Autoinflammatory Diseases (SAID) Autoinflammatory Alliance. 2013 http://www.nomidalliance.org/downloads/comparative_chart_front.pdf.
-
- Ferguson P, Chen S, Tayeh M, Ochoa L, Leal S, Pelet A, et al. Homozygous mutations in LPIN2are responsible for the syndrome of chronic recurrent multifocal osteomyelitis and congenital dyserythropoietic anaemia (Majeed syndrome) J Med Genet. 2005;42:551–7. doi: 10.1136/jmg.2005.030759. - DOI - PMC - PubMed
-
- Fukushima Y, Obara K, Hirata H, Sugiyama K, Fukuda T, Takabe K. Three Japanese patients(mother and two children) with familial Mediterranean fever associated with compoundheterozygosity for L110P/E148Q/M694I and anautosomal true dominant inheritance pattern. Asian Pac J Allergy Immunol. 2013;31:325–9. doi: 10.12932/AP0244.31.4.2013. - DOI - PubMed
LinkOut - more resources
Full Text Sources
