

Focal therapy versus robot-assisted partial nephrectomy in the management of clinical T1 renal masses: A systematic review and meta-analysis
- PMID: 30407321
- PMCID: PMC6250551
- DOI: 10.1097/MD.0000000000013102
Focal therapy versus robot-assisted partial nephrectomy in the management of clinical T1 renal masses: A systematic review and meta-analysis
Abstract
Background: Robot-assisted partial nephrectomy (RPN) and focal therapy (FT) have both been successfully employed in the management of small renal masses. However, despite this being the era of minimally invasive surgery, few comparative studies exist on RPN and FT. The aim of our study is to review perioperative, renal functional and oncologic outcomes of FT and RPN in cT1 renal masses.
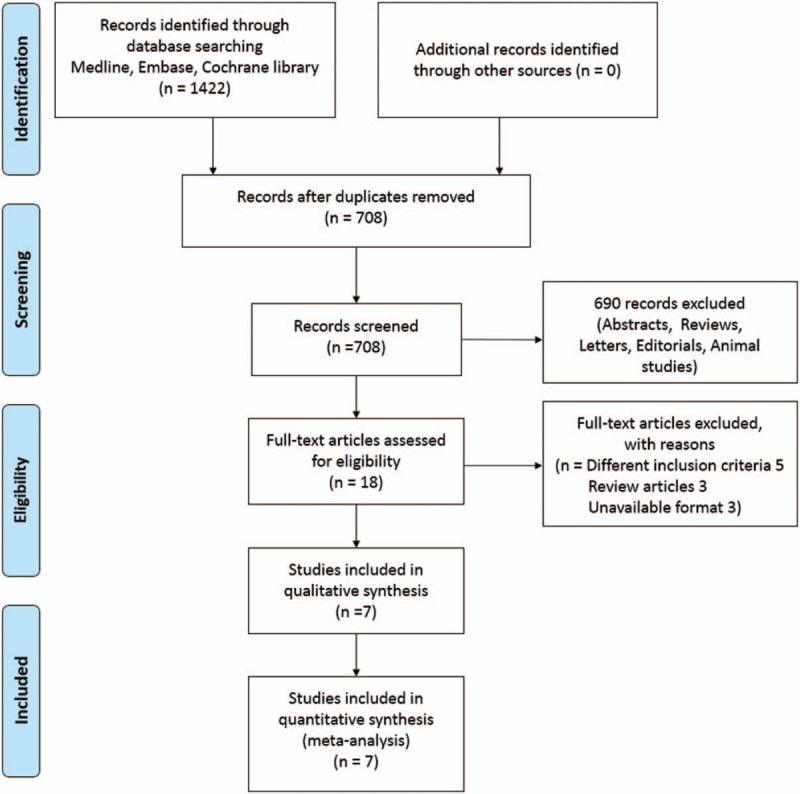
Methods: Literature published in Medline, EMBASE, and Cochrane Library databases up to April 22, 2018, was systematically searched. We included literature comparing outcomes of FT (radiofrequency ablation, cryoablation, microwave ablation, and irreversible electroporation) and RPN. Studies that reported only on laparoscopic partial nephrectomy or open partial nephrectomy, and review articles, editorials, letters, or cost analyses were excluded. In total, data from 1166 patients were included.
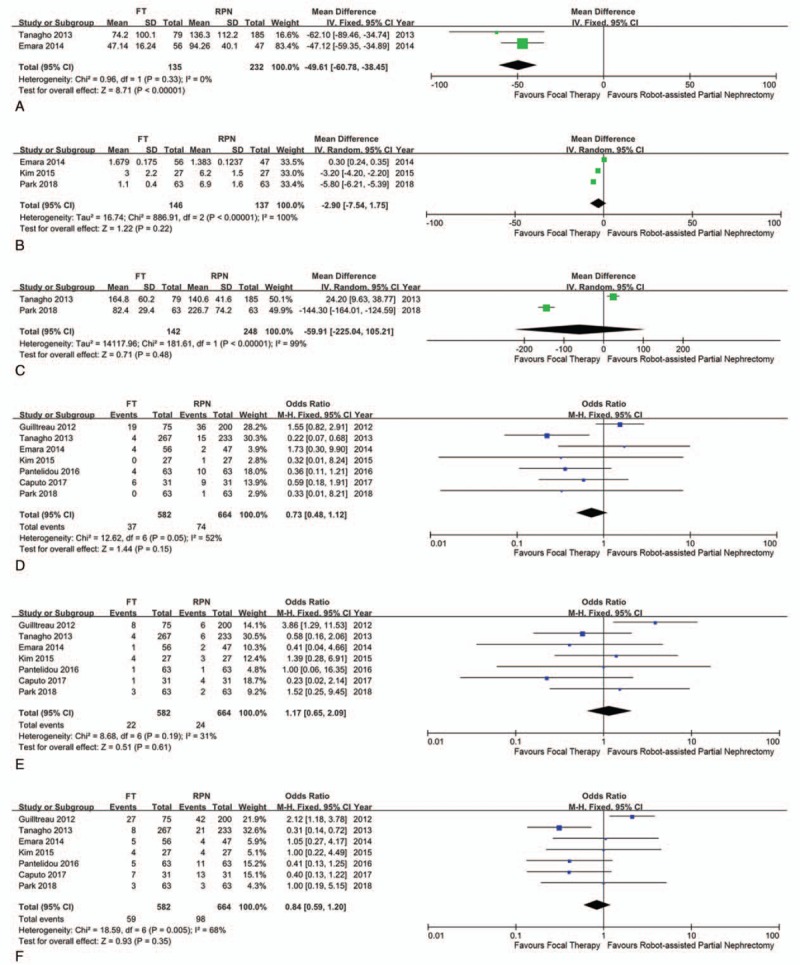
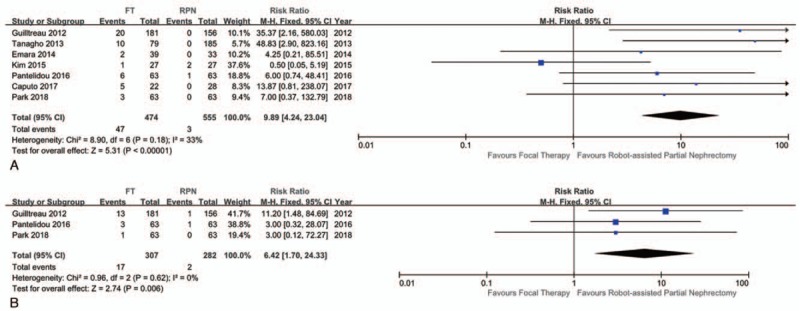
Results: From 858 total articles, 7 nonrandomized, observational studies were included. Compared with RPN, FT was associated with a significantly lower decrease of estimated glomerular filtration rate (weighted mean difference [WMD] -8.06 mL/min/1.73 m; confidence interval [CI] -15.85 to -0.26; P = .04), and lower estimated blood loss (WMD -49.61 mL; CI -60.78 to -38.45; P < .001). However, patients who underwent FT had a significantly increased risk of local recurrence (risk ratio [RR] 9.89; CI 4.24-23.04; P < .001) and distant metastasis (RR 6.42; CI 1.70-24.33; P = .006). However, operative times, lengths of stay, and complication rates were revealed to be similar between FT and RPN.
Conclusion: RPN has a substantial advantage in preventing cancer recurrence. However, in the era of minimally invasive surgery, FT has advantages in renal function preservation and less bleeding. Long-term follow-up for survival rates and comparative analysis of microwave ablation and irreversible electroporation are needed to extend FT for patients with significant morbidities and for those who need sufficient renal function preservation with minimal bleeding.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures

References
-
- Campbell SC, Novick AC, Belldegrun A, et al. Guideline for management of the clinical T1 renal mass. J Urol 2009;182:1271–9. - PubMed
-
- Ficarra V, Novara G, Secco S, et al. Preoperative aspects and dimensions used for an anatomical (PADUA) classification of renal tumours in patients who are candidates for nephron-sparing surgery. Eur Urol 2009;56:786–93. - PubMed
-
- Choi JE, You JH, Kim DK, et al. Comparison of perioperative outcomes between robotic and laparoscopic partial nephrectomy: a systematic review and meta-analysis. Eur Urol 2015;67:891–901. - PubMed
-
- Johnson BA, Cadeddu JA. Current opinion in urology 2017: focal therapy of small renal lesions. Curr Opin Urol 2018;28:166–71. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
