

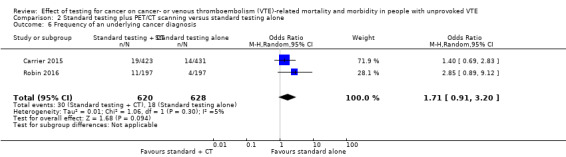
Effect of testing for cancer on cancer- or venous thromboembolism (VTE)-related mortality and morbidity in people with unprovoked VTE
- PMID: 30407621
- PMCID: PMC6517248
- DOI: 10.1002/14651858.CD010837.pub4
Effect of testing for cancer on cancer- or venous thromboembolism (VTE)-related mortality and morbidity in people with unprovoked VTE
Update in
-
Effect of testing for cancer on cancer- or venous thromboembolism (VTE)-related mortality and morbidity in people with unprovoked VTE.Cochrane Database Syst Rev. 2021 Oct 1;10(10):CD010837. doi: 10.1002/14651858.CD010837.pub5. Cochrane Database Syst Rev. 2021. PMID: 34597414 Free PMC article.
Abstract
Background: Venous thromboembolism (VTE) is a collective term for two conditions: deep vein thrombosis (DVT) and pulmonary embolism (PE). A proportion of people with VTE have no underlying or immediately predisposing risk factors and the VTE is referred to as unprovoked. Unprovoked VTE can often be the first clinical manifestation of an underlying malignancy. This has raised the question of whether people with an unprovoked VTE should be investigated for an underlying cancer. Treatment for VTE is different in cancer and non-cancer patients and a correct diagnosis would ensure that people received the optimal treatment for VTE to prevent recurrence and further morbidity. Furthermore, an appropriate cancer diagnosis at an earlier stage could avoid the risk of cancer progression and lead to improvements in cancer-related mortality and morbidity. This is an update of a review first published in 2015.
Objectives: To determine whether testing for undiagnosed cancer in people with a first episode of unprovoked VTE (DVT of the lower limb or PE) is effective in reducing cancer or VTE-related mortality and morbidity and to determine which tests for cancer are best at identifying treatable cancers early.
Search methods: The Cochrane Vascular Information Specialist searched the Cochrane Vascular Specialised Register, CENTRAL, MEDLINE, Embase and CINAHL databases and World Health Organization International Clinical Trials Registry Platform and ClinicalTrials.gov trials registers to 11 July 2018. We also undertook reference checking to identify additional studies.
Selection criteria: Randomised and quasi-randomised trials in which people with an unprovoked VTE were allocated to receive specific tests for identifying cancer or clinically indicated tests only were eligible for inclusion. Primary outcomes included all-cause mortality, cancer-related mortality and VTE-related mortality.
Data collection and analysis: Two review authors independently selected studies, assessed risk of bias and extracted data. We resolved any disagreements by discussion.
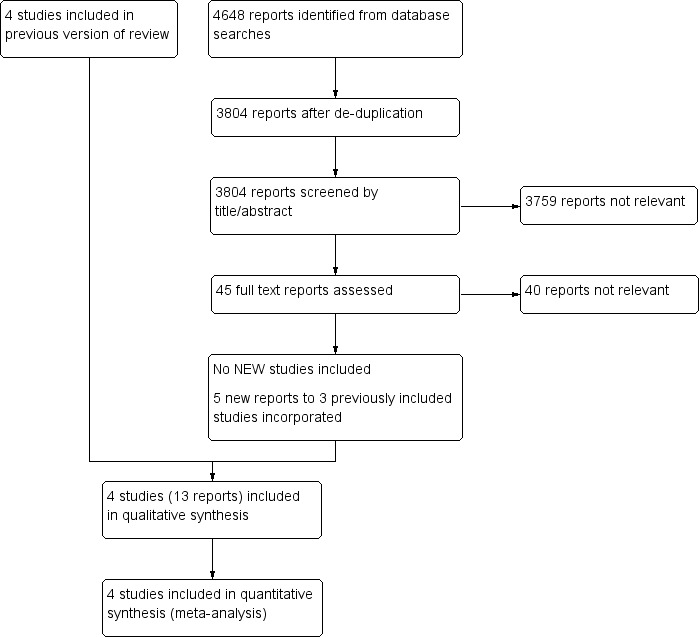
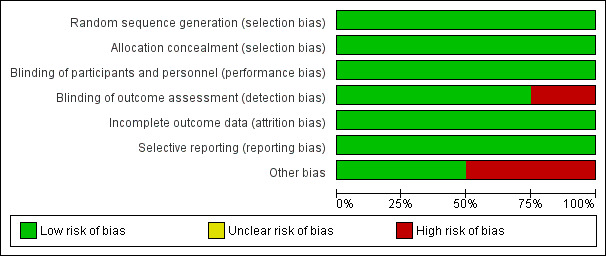
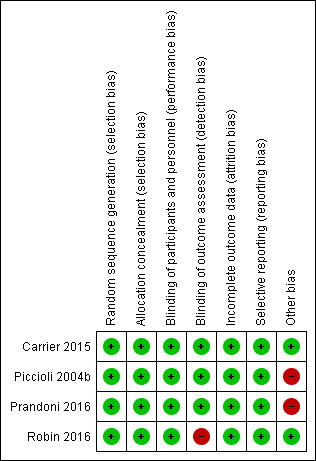
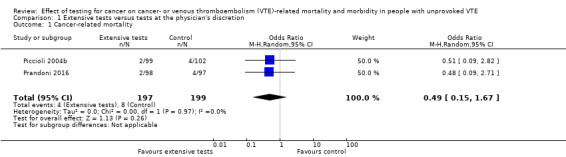
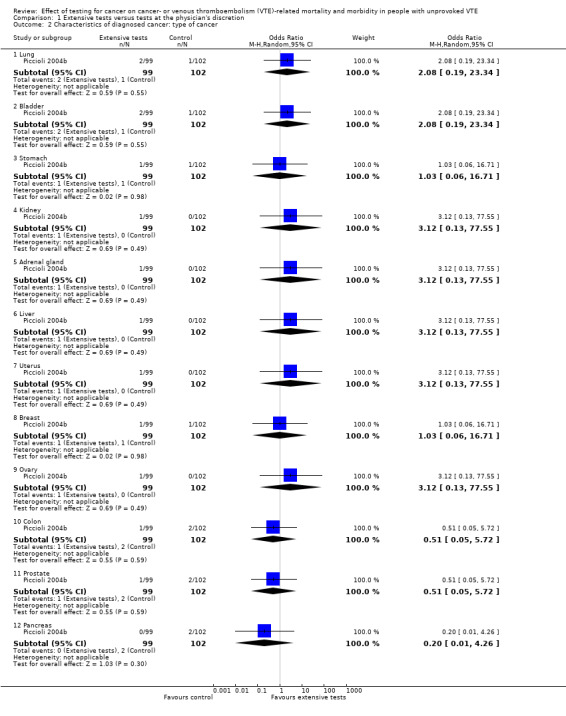
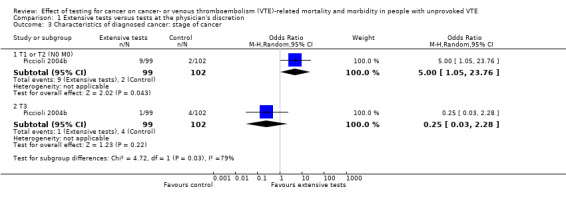
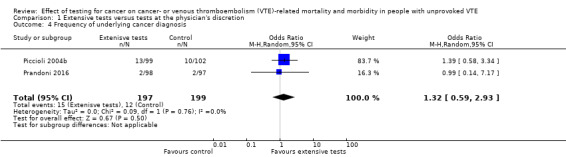
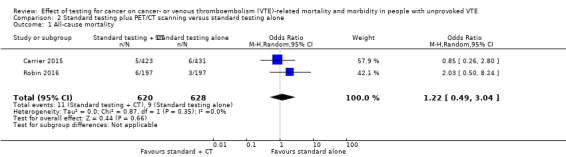
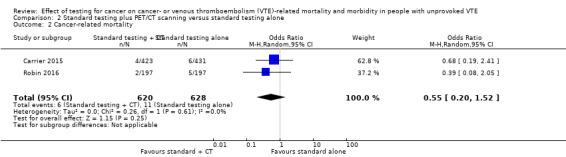
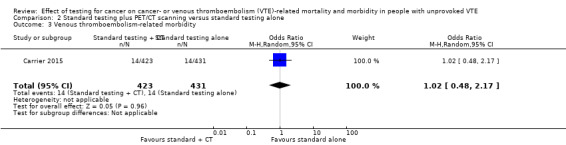
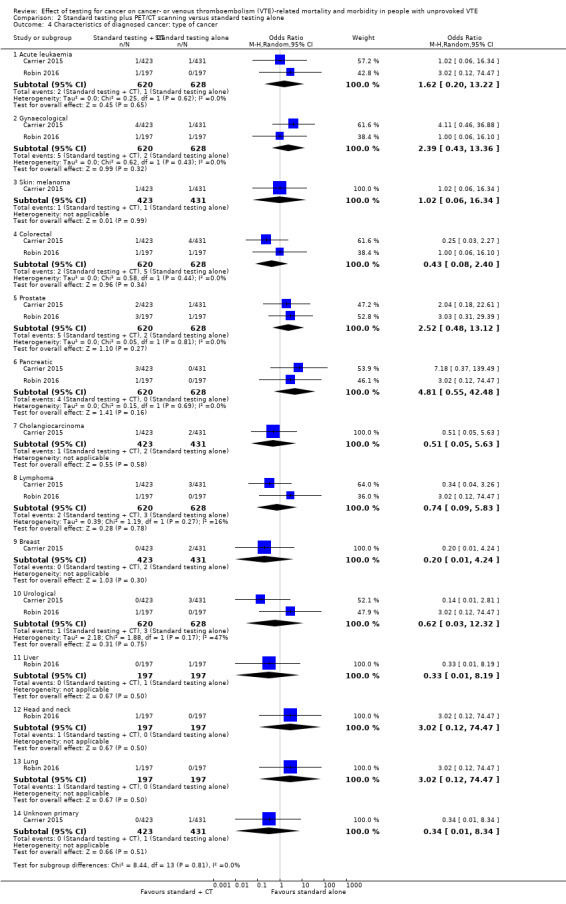
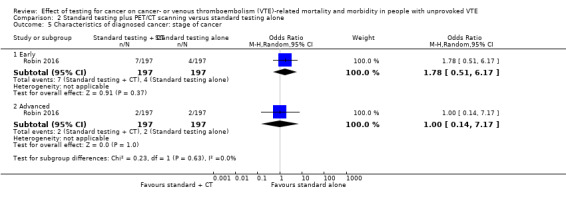
Main results: No new studies were identified for this 2018 update. In total, four studies with 1644 participants are included. Two studies assessed the effect of extensive tests including computed tomography (CT) scanning versus tests at the physician's discretion, while the other two studies assessed the effect of standard testing plus positron emission tomography (PET)/CT scanning versus standard testing alone. For extensive tests including CT versus tests at the physician's discretion, the quality of the evidence, as assessed according to GRADE, was low due to risk of bias (early termination of the studies). When comparing standard testing plus PET/CT scanning versus standard testing alone, the quality of evidence was moderate due to a risk of detection bias. The quality of the evidence was downgraded further as detection bias was present in one study with a low number of events.When comparing extensive tests including CT versus tests at the physician's discretion, pooled analysis on two studies showed that testing for cancer was consistent with either benefit or no benefit on cancer-related mortality (odds ratio (OR) 0.49, 95% confidence interval (CI) 0.15 to 1.67; 396 participants; 2 studies; P = 0.26; low-quality evidence). One study (201 participants) showed that, overall, malignancies were less advanced at diagnosis in extensively tested participants than in participants in the control group. In total, 9/13 participants diagnosed with cancer in the extensively tested group had a T1 or T2 stage malignancy compared to 2/10 participants diagnosed with cancer in the control group (OR 5.00, 95% CI 1.05 to 23.76; P = 0.04; low-quality evidence). There was no clear difference in detection of advanced stages between extensive tests versus tests at the physician's discretion: one participant in the extensively tested group had stage T3 compared with four participants in the control group (OR 0.25, 95% CI 0.03 to 2.28; P = 0.22; low-quality evidence). In addition, extensively tested participants were diagnosed earlier than control group (mean: 1 month with extensive tests versus 11.6 months with tests at physician's discretion to cancer diagnosis from the time of diagnosis of VTE). Extensive testing did not increase the frequency of an underlying cancer diagnosis (OR 1.32, 95% CI 0.59 to 2.93; 396 participants; 2 studies; P = 0.50; low-quality evidence). Neither study measured all-cause mortality, VTE-related morbidity and mortality, complications of anticoagulation, adverse effects of cancer tests, participant satisfaction or quality of life.When comparing standard testing plus PET/CT screening versus standard testing alone, standard testing plus PET/CT screening was consistent with either benefit or no benefit on all-cause mortality (OR 1.22, 95% CI 0.49 to 3.04; 1248 participants; 2 studies; P = 0.66; moderate-quality evidence), cancer-related mortality (OR 0.55, 95% CI 0.20 to 1.52; 1248 participants; 2 studies; P = 0.25; moderate-quality evidence) or VTE-related morbidity (OR 1.02, 95% CI 0.48 to 2.17; 854 participants; 1 study; P = 0.96; moderate-quality evidence). Regarding stage of cancer, there was no clear difference for detection of early (OR 1.78, 95% 0.51 to 6.17; 394 participants; 1 study; P = 0.37; low-quality evidence) or advanced (OR 1.00, 95% CI 0.14 to 7.17; 394 participants; 1 study; P = 1.00; low-quality evidence) stages of cancer. There was also no clear difference in the frequency of an underlying cancer diagnosis (OR 1.71, 95% CI 0.91 to 3.20; 1248 participants; 2 studies; P = 0.09; moderate-quality evidence). Time to cancer diagnosis was 4.2 months in the standard testing group and 4.0 months in the standard testing plus PET/CT group (P = 0.88). Neither study measured VTE-related mortality, complications of anticoagulation, adverse effects of cancer tests, participant satisfaction or quality of life.
Authors' conclusions: Specific testing for cancer in people with unprovoked VTE may lead to earlier diagnosis of cancer at an earlier stage of the disease. However, there is currently insufficient evidence to draw definitive conclusions concerning the effectiveness of testing for undiagnosed cancer in people with a first episode of unprovoked VTE (DVT or PE) in reducing cancer- or VTE-related morbidity and mortality. The results could be consistent with either benefit or no benefit. Further good-quality large-scale randomised controlled trials are required before firm conclusions can be made.
Conflict of interest statement
LR: none known. SEY: none known. CB: none known. GS: none known. RA: none known.
As CB is based within Cochrane Vascular, editorial tasks for this update were carried out by other members of the Cochane Vascular editorial team.
Figures
Update of
-
Effect of testing for cancer on cancer- and venous thromboembolism (VTE)-related mortality and morbidity in people with unprovoked VTE.Cochrane Database Syst Rev. 2017 Aug 23;8(8):CD010837. doi: 10.1002/14651858.CD010837.pub3. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2018 Nov 08;11:CD010837. doi: 10.1002/14651858.CD010837.pub4. PMID: 28832905 Free PMC article. Updated.
Similar articles
-
Effect of testing for cancer on cancer- or venous thromboembolism (VTE)-related mortality and morbidity in people with unprovoked VTE.Cochrane Database Syst Rev. 2021 Oct 1;10(10):CD010837. doi: 10.1002/14651858.CD010837.pub5. Cochrane Database Syst Rev. 2021. PMID: 34597414 Free PMC article.
-
Effect of testing for cancer on cancer- and venous thromboembolism (VTE)-related mortality and morbidity in people with unprovoked VTE.Cochrane Database Syst Rev. 2017 Aug 23;8(8):CD010837. doi: 10.1002/14651858.CD010837.pub3. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2018 Nov 08;11:CD010837. doi: 10.1002/14651858.CD010837.pub4. PMID: 28832905 Free PMC article. Updated.
-
Effect of testing for cancer on cancer- and venous thromboembolism (VTE)-related mortality and morbidity in patients with unprovoked VTE.Cochrane Database Syst Rev. 2015 Mar 6;(3):CD010837. doi: 10.1002/14651858.CD010837.pub2. Cochrane Database Syst Rev. 2015. Update in: Cochrane Database Syst Rev. 2017 Aug 23;8:CD010837. doi: 10.1002/14651858.CD010837.pub3. PMID: 25749503 Updated.
-
Primary prophylaxis for venous thromboembolism in people undergoing major amputation of the lower extremity.Cochrane Database Syst Rev. 2020 Jul 21;7(7):CD010525. doi: 10.1002/14651858.CD010525.pub3. Cochrane Database Syst Rev. 2020. PMID: 32692430 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
Cited by
-
Pulmonary embolism.Clin Med (Lond). 2019 Jul;19(4):357-358. doi: 10.7861/clinmedicine.19-4-357a. Clin Med (Lond). 2019. PMID: 31308127 Free PMC article. No abstract available.
-
An incidental finding of testicular seminoma in the context of acute pulmonary embolism: a case report.J Med Case Rep. 2021 Jul 20;15(1):354. doi: 10.1186/s13256-021-02925-z. J Med Case Rep. 2021. PMID: 34281593 Free PMC article.
-
Effect of testing for cancer on cancer- or venous thromboembolism (VTE)-related mortality and morbidity in people with unprovoked VTE.Cochrane Database Syst Rev. 2021 Oct 1;10(10):CD010837. doi: 10.1002/14651858.CD010837.pub5. Cochrane Database Syst Rev. 2021. PMID: 34597414 Free PMC article.
-
CT imaging for occult malignancy in patients with unprovoked venous thromboembolism (VTE) in a tertiary centre: is it worthwhile?Ir J Med Sci. 2023 Dec;192(6):3081-3086. doi: 10.1007/s11845-023-03317-6. Epub 2023 Feb 27. Ir J Med Sci. 2023. PMID: 36849651 Free PMC article.
-
A review of 117 cases of unprovoked pulmonary embolism and further investigation in patients over 40.Clin Med (Lond). 2020 Mar;20(Suppl 2):s64. doi: 10.7861/clinmed.20-2-s64. Clin Med (Lond). 2020. PMID: 32409382 Free PMC article. Review. No abstract available.
References
References to studies included in this review
Carrier 2015 {published data only}
-
- Carrier M, Lazo‐Langner A, Shivakumar S, Tagalakis V, Zarychanski R, Solymoss S, et al. Screening for occult cancer in unprovoked venous thromboembolism. New England Journal of Medicine 2015;373(8):697‐704. - PubMed
-
- Coyle K, Carrier M, Lazo‐Langner A, Shivakumar S, Zarychanski R, Tagalakis V, et al. Cost effectiveness of the addition of a comprehensive CT scan to the abdomen and pelvis for the detection of cancer after unprovoked venous thromboembolism. Thrombosis Research 2017;151:67‐71. - PubMed
Piccioli 2004b {published data only}
-
- Otten HM, Prins MH. A number needed to screen and cost‐effectiveness analysis of the SOMIT‐data. Haemostasis 2001;31 Suppl 1:40‐2. - PubMed
-
- Piccioli A, Lensing AWA, Prins MH, Falanga A, Scannapieco GL, Ieran M, et al. Extensive screening for occult malignant disease in idiopathic venous thromboembolism: a prospective randomized clinical trial. Journal of Thrombosis and Haemostasis 2004;2:884‐9. - PubMed
Prandoni 2016 {published data only}
-
- Piccioli A. The value of CT scanning for detection of occult cancer in patients with idiopathic VTE. Cancer, thrombosis and low‐molecular‐weight heparins (dare.uva.nl/record/1/465654 (accessed June 2016)). Amsterdam (the Netherlands): University of Amsterdam, 2015.
-
- Piccioli A, Bernardi E, Dalla Valle F, Visona A, Tropeano F, Bova C, et al. The value of CT‐scanning for detection of occult cancer in patients with unprovoked venous thromboembolism. The D'Acquapendente study. Journal of Thrombosis and Haemostasis 2013;11 (Suppl 2):50‐1.
-
- Piccioli A, Bernardi E, Dalla Valle F, Visonà A, Tropeano PF, Bova C, et al. The value of thoraco‐abdominal CT scanning for the detection of occult cancer in patients with unprovoked venous thromboembolism. A randomized study. Thrombosis Research 2012;129 Suppl 1:S155‐94.
-
- Prandoni P, Bernardi E, Dalla Valle F, Visona A, Tropeano PF, Bova C, et al. Extensive computed tomography versus limited screening for detection of occult cancer in unprovoked venous thromboembolism: a multicenter, controlled, randomized clinical trial. Blood Transfusion 2016;14(Suppl 5):s745‐6. - PubMed
-
- Prandoni P, Bernardi E, Valle FD, Visona A, Tropeano PF, Bova C, et al. Extensive computed tomography versus limited screening for detection of occult cancer in unprovoked venous thromboembolism: a multicenter, controlled, randomized clinical trial. Seminars in Thrombosis and Hemostasis 2016;42(8):884‐90. - PubMed
Robin 2016 {published data only}
-
- Robin P, Roux PY, Moigne E, Planquette B, Prevot‐Bitot N, Roy P, et al. Additional testing following screening strategies for occult malignancy diagnosis in patients with unprovoked venous thromboembolism. Thrombosis Research 2017;155:6‐9. - PubMed
-
- Robin P, Roux PY, Planquette B, Accassat S, Roy PM, Couturaud F, et al. Limited screening with versus without (18)F‐fluorodeoxyglucose PET/CT for occult malignancy in unprovoked venous thromboembolism: an open‐label randomised controlled trial. Lancet Oncology 2016;17(2):193‐9. - PubMed
-
- Robin P, Roux PY, Tromeur C, Planquette B, Prevot‐Bitot N, Lavigne C, et al. Risk factors of occult malignancy in patients with unprovoked venous thromboembolism. Thrombosis Research 2017;159:48‐51. - PubMed
Additional references
Atkins 2004
Baron 1998
-
- Baron JA, Gridley G, Weiderpass E, Nyren O, Linet M. Venous thromboembolism and cancer. Lancet 1998;351(9109):1077‐80. - PubMed
Bick 1978
-
- Bick RL. Alterations of hemostasis associated with malignancy: etiology, pathophysiology, diagnosis and management. Seminars in Thrombosis and Hemostasis 1978;5(1):1‐26. - PubMed
Buthiau 2003
-
- Buthiau D, Rixe O, Spano JP, Nizri D, Delgado M, Gutierrez M, et al. New imaging techniques in oncology. European Journal of Cancer Supplements 2003;1(2):28‐42.
Carrier 2014
-
- Carrier M, Cameron C, Delluc A, Castellucci L, Khorana AA, Lee AY. Efficacy and safety of anticoagulant therapy for the treatment of acute cancer‐associated thrombosis: a systematic review and meta‐analysis. Thrombosis Research 2014;134(6):1214‐9. - PubMed
Chen 2004
-
- Chen YK, Ding HJ, Su CT, Shen YY, Chen LK, Liao AC, et al. Application of PET and PET/CT imaging for cancer screening. Anticancer Research 2004;24(6):4103‐8. - PubMed
Chin 2008
-
- Chin BB. Clinical utility of combined 18F‐fluor‐2‐deoxyglucose positron emission tomography‐computed tomography in the evaluation of gastrointestinal malignancies. Current Medical Imaging Reviews 2008;4(4):255‐69.
Deeks 2011
-
- Deeks JJ, Higgins JPT, Altman DG. Chapter 9: Analysing data and undertaking meta‐analyses. In: Higgins JPT, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Higgins 2011
-
- Higgins JPT, Altman DG, Sterne JAC. Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Kakkar 2003
-
- Kakkar AK, Levine M, Pinedo HM, Wolff R, Wong J. Venous thrombosis in cancer patients: insights from the FRONTLINE survey. Oncologist 2003;8(4):381‐8. - PubMed
Klein 2017
-
- Klein A, Shepshelovich D, Spectre G, Goldvaser H, Raanani P, Gafter‐Gvili A. Screening for occult cancer in idiopathic venous thromboembolism ‐ systemic review and meta‐analysis. European Journal of Internal Medicine 2017;42:74‐80. - PubMed
Lee 2003a
-
- Lee AY, Levine MN. Venous thromboembolism and cancer: risks and outcomes. Circulation 2003;107(23 Suppl 1):I17‐21. - PubMed
Lee 2003b
-
- Lee AYY, Levine MN, Baker RI, Bowden C, Kakkar AK, Prins M, et al. Low‐molecular‐weight heparin versus a coumarin for the prevention of recurrent venous thromboembolism in patients with cancer. New England Journal of Medicine 2003;349(2):146‐53. - PubMed
Lefebvre 2011
-
- Lefebvre C, Manheimer E, Glanville J. Chapter 6: Searching for studies. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Levitan 1999
-
- Levitan N, Dowlati A, Remick SC, Tahsildar HI, Sivinski LD, Beyth R, et al. Rates of initial and recurrent thromboembolic disease among patients with malignancy versus those without malignancy. Risk analysis using Medicare claims data. Medicine (Baltimore) 1999;78(5):285‐91. - PubMed
NICE 2012
-
- National Institute for Health and Care Excellence. Venous thromboembolic diseases: the management of venous thromboembolic diseases and the role of thrombophilia testing. NICE Clinical Guideline 144. www.nice.org.uk/guidance/cg144 (accessed 2 August 2017).
Piccioli 2004a
-
- Piccioli A, Lensing AW, Prins MH, Falanga A, Scannapieco GL, Ieran M, et al. SOMIT Investigators Group. Extensive screening for occult malignant disease in idiopathic venous thromboembolism: a prospective randomized clinical trial. Journal of Thrombosis and Haemostasis 2004;2(6):884‐9. - PubMed
Prandoni 1997
-
- Prandoni P, Piccioli A. Venous thromboembolism and cancer: a two‐way clinical association. Frontiers in Bioscience 1997;2:e12‐21. - PubMed
RevMan 2014 [Computer program]
-
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Schöder 2007
-
- Schöder H, Gönen M. Screening for cancer with PET and PET/CT: potential and limitations. Journal of Nuclear Medicine 2007;48(1):4S–18S. - PubMed
Sorensen 2000
-
- Sorensen HT, Mellemkjaer L, Olsen JH, Baron JA. Prognosis of cancers associated with venous thromboembolism. New England Journal of Medicine 2000;343:1846‐50. - PubMed
Sterne 2011
-
- Sterne JAC, Egger M, Moher D. Chapter 10: Addressing reporting biases. In: Higgins JPT, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
van Doormaal 2011
-
- Doormaal FF, Terpstra W, Griend R, Prins MH, Nijziel MR, Ree MA, et al. Is extensive screening for cancer in idiopathic venous thromboembolism warranted?. Journal of Thrombosis and Haemostasis 2011;9:79‐84. - PubMed
van Es 2017
-
- Es N, Gal G, Otten HM, Robin P, Piccioli A, Lecumberri R, et al. Screening for occult cancer in patients with unprovoked venous thromboembolism. Annals of Internal Medicine 2017;167(6):410‐7. - PubMed
Vedovati 2015
-
- Vedovati MC, Germini F, Agnelli G, Becattini C. Direct oral anticoagulants in patients with VTE and cancer: a systematic review and meta‐analysis. Chest 2015;147(2):475‐83. - PubMed
White 2005
-
- White RH, Chew HK, Zhou H, Parikh‐Patel A, Harris D, Harvey D, et al. Incidence of venous thromboembolism in the year before the diagnosis of cancer in 528,693 adults. Archives of Internal Medicine 2005;165(15):1782‐7. - PubMed
Zhou 2017
-
- Zhou M, Zhang L, Ding Y, Wang Y, Yan D, Lin C, et al. Extensive screening for occult malignancy in unprovoked venous thromboembolism: a meta‐analysis. Thrombosis Research 2017;157:147‐53. - PubMed
References to other published versions of this review
Robertson 2013
Robertson 2015
Robertson 2017
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical