

Health Care Barriers to Provision of Long-Acting Reversible Contraception in Wisconsin
- PMID: 30407764
- PMCID: PMC6734562
Health Care Barriers to Provision of Long-Acting Reversible Contraception in Wisconsin
Abstract
Introduction: Long-acting reversible contraceptives (LARC), specifically implants and intrauterine devices (IUD), are highly effective, low maintenance forms of birth control. Practice guidelines from the American College of Obstetricians and Gynecologists, American Academy of Family Physicians, and American Academy of Pediatrics recommend that LARC be considered first-line birth control for most women; however, uptake remains low. In this study, we sought to understand practices and barriers to provision of LARC in routine and immediate postpartum settings as they differ between specialties.
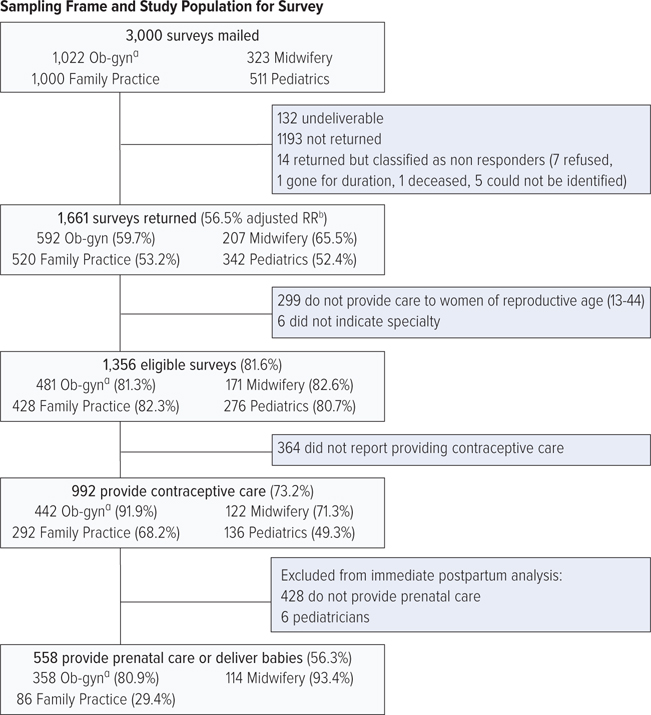
Methods: We surveyed 3,000 Wisconsin physicians and advanced-practice providers in obstetrics-gynecology/women's health (Ob-gyn), family medicine, pediatrics, and midwifery to assess practices and barriers (56.5% response rate). This analysis is comprised of contraceptive care providers (n=992); statistical significance was tested using chi-square and 2-sample proportions tests.
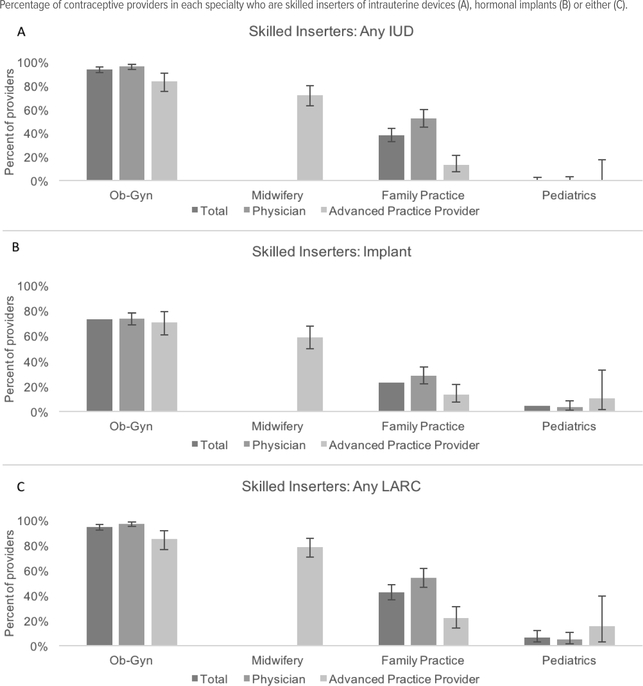
Results: More providers working Ob-gyn (94.3%) and midwifery (78.7%) were skilled providers of LARC methods than those in family medicine (42.5%) and pediatrics (6.6%) (P < .0001). Lack of insertion skill was the most-cited barrier to routine provision among family medicine (31.1%) and pediatric (72.1%) providers. Among prenatal/delivery providers, over 50% across all specialties reported lack of device availability on-site as a barrier to immediate postpartum LARC provision; organizational practices also were commonly reported barriers.
Conclusions: Gaps in routine and immediate postpartum LARC practice were strongly related to specialty, and providers' experience heightened barriers to immediate postpartum compared to routine insertion. Skills training targeting family medicine and pediatric providers would enable broader access to LARC. Organizational barriers to immediate postpartum LARC provision impact many providers.
Copyright© Wisconsin Medical Society.
Figures
Similar articles
-
Adherence to Recommended Practices for Provision of Long-Acting Reversible Contraception Among Providers in a Large U.S. Health Care System.J Womens Health (Larchmt). 2020 Dec;29(12):1586-1595. doi: 10.1089/jwh.2019.8169. Epub 2020 Jul 13. J Womens Health (Larchmt). 2020. PMID: 32667847 Free PMC article.
-
Familiarity with Long-acting Reversible Contraceptives among Obstetrics and Gynecology, Family Medicine, and Pediatrics Residents: Results of a 2015 National Survey and Implications for Contraceptive Provision for Adolescents.J Pediatr Adolesc Gynecol. 2018 Feb;31(1):40-44. doi: 10.1016/j.jpag.2017.09.007. Epub 2017 Sep 21. J Pediatr Adolesc Gynecol. 2018. PMID: 28942106
-
Implementing best practices for the provision of long-acting reversible contraception: a survey of obstetrician-gynecologists.Contraception. 2019 Aug;100(2):123-127. doi: 10.1016/j.contraception.2019.03.053. Epub 2019 Apr 11. Contraception. 2019. PMID: 30981843
-
Effective, recommended, underutilized: a review of the literature on barriers to adolescent usage of long-acting reversible contraceptive methods.Curr Opin Pediatr. 2018 Oct;30(5):683-688. doi: 10.1097/MOP.0000000000000663. Curr Opin Pediatr. 2018. PMID: 30028744 Review.
-
Patients and providers' knowledge, attitudes, and beliefs regarding immediate postpartum long-acting reversible contraception: a systematic review.Women Health. 2020 Feb;60(2):179-196. doi: 10.1080/03630242.2019.1616042. Epub 2019 May 23. Women Health. 2020. PMID: 31122167
Cited by
-
Barriers for multiparous women to using long-term contraceptive methods in Southeast Asia: case study in Philippines and Indonesia.BMC Public Health. 2022 Jul 27;22(1):1425. doi: 10.1186/s12889-022-13844-z. BMC Public Health. 2022. PMID: 35883076 Free PMC article.
-
Short-acting hormonal contraceptive continuation among low-income postpartum women in Texas.Contracept X. 2020 Dec 28;3:100052. doi: 10.1016/j.conx.2020.100052. eCollection 2021. Contracept X. 2020. PMID: 33490950 Free PMC article.
-
Opposition to Pharmacist Contraception Services: Evidence for Rebuttal.Pharmacy (Basel). 2020 Sep 23;8(4):176. doi: 10.3390/pharmacy8040176. Pharmacy (Basel). 2020. PMID: 32977545 Free PMC article.
-
Knowledge, beliefs and practices of nurses with long-acting reversible contraception, Cape Town.Afr J Prim Health Care Fam Med. 2023 May 24;15(1):e1-e8. doi: 10.4102/phcfm.v15i1.3571. Afr J Prim Health Care Fam Med. 2023. PMID: 37265159 Free PMC article.
-
Integrating long-acting reversible contraceptives into primary care internal medicine practices: A clinical innovation to reduce wait time.Womens Health (Lond). 2023 Jan-Dec;19:17455057231219569. doi: 10.1177/17455057231219569. Womens Health (Lond). 2023. PMID: 38130094 Free PMC article.
References
-
- Sonfield A, Kost K. Public costs from unintended pregnancies and the role of public insurance programs in paying for pregnancy-related care: national and state estimates for 2010. Guttmacher Institute; https://www.guttmacher.org/pubs/public-costs-of-UP-2010.pdf. Published February 2015. Accessed December 1, 2016.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous