

Impact of fee subsidy policy on perinatal health in a low-resource setting: A quasi-experimental study
- PMID: 30408129
- PMCID: PMC6224097
- DOI: 10.1371/journal.pone.0206978
Impact of fee subsidy policy on perinatal health in a low-resource setting: A quasi-experimental study
Abstract
Background: A national subsidy policy was introduced in 2007 in Burkina Faso to improve financial accessibility to facility-based delivery. In this article, we estimated the effects of reducing user fees on institutional delivery and neonatal mortality, immediately and three years after the introduction of the policy.
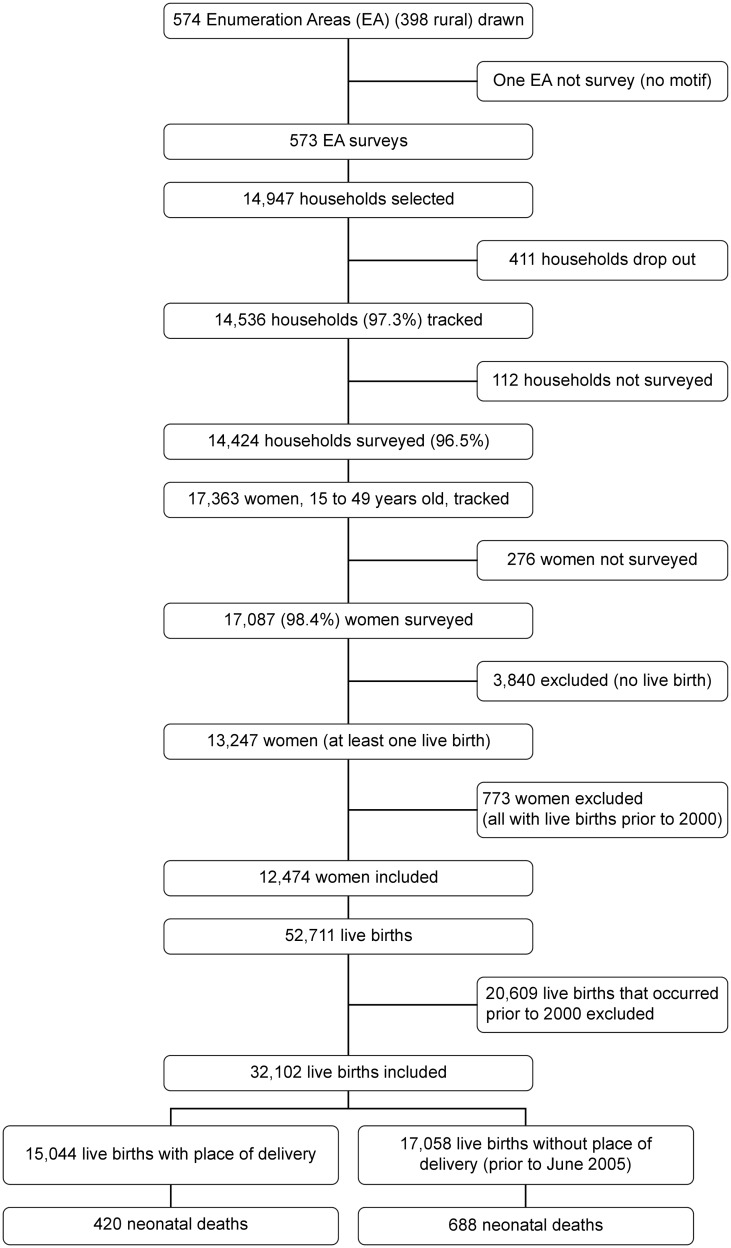
Methods: The study was based on a quasi-experimental design. We used data obtained from the 2010 Demographic and Health Survey, including survival information for 32,102 live-born infants born to 12,474 women. We used a multilevel Poisson regression model with robust variances to control for secular trends in outcomes between the period before the introduction of the policy (1 January, 2007) and the period after. In sensitivity analyses, we used two different models according to the different definitions of the period "before" and the period "after".
Results: Immediately following its introduction, the subsidy policy was associated with increases in institutional deliveries by 4% (RR = 1.04, 95% CI: 0.98-1.10) in urban areas and by 12% (RR = 1.12, 95% CI: 1.04-1.20) in rural areas. The results showed similar patterns in sensitivity analyses. This effect was particularly marked among rural clusters with low institutional delivery rates at baseline (RR = 1.44, 95% CI: 1.33-1.55). It was persistent for 42 months after the introduction of the policy but these increases were not statistically significant. At 42 months, the delivery rates had increased by 26% in rural areas (RR = 1.26; 95% CI: 0.86-1.86) and 13% (RR = 1.13; 95% CI: 0.88-1.46) in urban areas. There was no evidence of a significant decrease in neonatal mortality rates.
Conclusion: The delivery subsidy implemented in Burkina Faso is associated with short-term increases in health facility deliveries. This policy has been particularly beneficial for rural households.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Effect of a policy to reduce user fees on the rate of skilled birth attendance across socioeconomic strata in Burkina Faso.Health Policy Plan. 2016 May;31(4):462-71. doi: 10.1093/heapol/czv088. Epub 2015 Oct 8. Health Policy Plan. 2016. PMID: 26453087 Free PMC article.
-
The obstetric care subsidy policy in Burkina Faso: what are the effects after five years of implementation? Findings of a complex evaluation.BMC Pregnancy Childbirth. 2016 Apr 21;16:84. doi: 10.1186/s12884-016-0875-2. BMC Pregnancy Childbirth. 2016. PMID: 27101897 Free PMC article.
-
Assessing the community-level impact of a decade of user fee policy shifts on health facility deliveries in Kenya, 2003-2014.Int J Equity Health. 2018 May 25;17(1):65. doi: 10.1186/s12939-018-0774-4. Int J Equity Health. 2018. PMID: 29801485 Free PMC article.
-
An assessment of the effect of user fee policy reform on facility-based deliveries in rural Zambia.BMC Res Notes. 2016 Dec 7;9(1):504. doi: 10.1186/s13104-016-2316-8. BMC Res Notes. 2016. PMID: 27927217 Free PMC article.
-
[Secular trends of institutional delivery rate in China from 1996 to 2015].Zhonghua Yi Xue Za Zhi. 2017 May 9;97(17):1337-1342. doi: 10.3760/cma.j.issn.0376-2491.2017.17.014. Zhonghua Yi Xue Za Zhi. 2017. PMID: 28482438 Chinese.
Cited by
-
The impact of the obstetrical risk insurance scheme in Mauritania on maternal healthcare utilization: a propensity score matching analysis.Health Policy Plan. 2020 May 1;35(4):388-398. doi: 10.1093/heapol/czz150. Health Policy Plan. 2020. PMID: 32003810 Free PMC article.
-
Financing for equity for women's, children's and adolescents' health in low- and middle-income countries: A scoping review.PLOS Glob Public Health. 2024 Sep 12;4(9):e0003573. doi: 10.1371/journal.pgph.0003573. eCollection 2024. PLOS Glob Public Health. 2024. PMID: 39264949 Free PMC article.
-
Effect of cost-reduction interventions on facility-based deliveries in Burkina Faso: a controlled interrupted time-series study with multiple non-equivalent dependent variables.J Epidemiol Community Health. 2023 Mar;77(3):133-139. doi: 10.1136/jech-2022-218794. Epub 2022 Dec 20. J Epidemiol Community Health. 2023. PMID: 36539278 Free PMC article.
References
-
- UNICEF. monitoring the situation of children and women: delivery care. New York: United Nations Children’s Fund, 2015.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
