

Increasing proportions of HIV-1 non-B subtypes and of NNRTI resistance between 2013 and 2016 in Germany: Results from the national molecular surveillance of new HIV-diagnoses
- PMID: 30408827
- PMCID: PMC6224275
- DOI: 10.1371/journal.pone.0206234
Increasing proportions of HIV-1 non-B subtypes and of NNRTI resistance between 2013 and 2016 in Germany: Results from the national molecular surveillance of new HIV-diagnoses
Abstract
Background: Molecular surveillance of newly diagnosed HIV-infections is important for tracking trends in circulating HIV-variants, including those with transmitted drug resistances (TDR) to sustain ART efficacy.
Methods: Dried serum spots (DSS) are received together with the statutory notification of a new diagnosis. 'Recent infections' (<155 days) classified by a 'recent infection test algorithm' (BED-CEIA and clinical data) are genotyped in HIV-protease (PR), reverse transcriptase (RT) and integrase (INT) to determine the HIV-1 subtype, to calculate prevalence and trends of TDR, to predict baseline susceptibility and to identify potential transmission clusters for resistant variants.
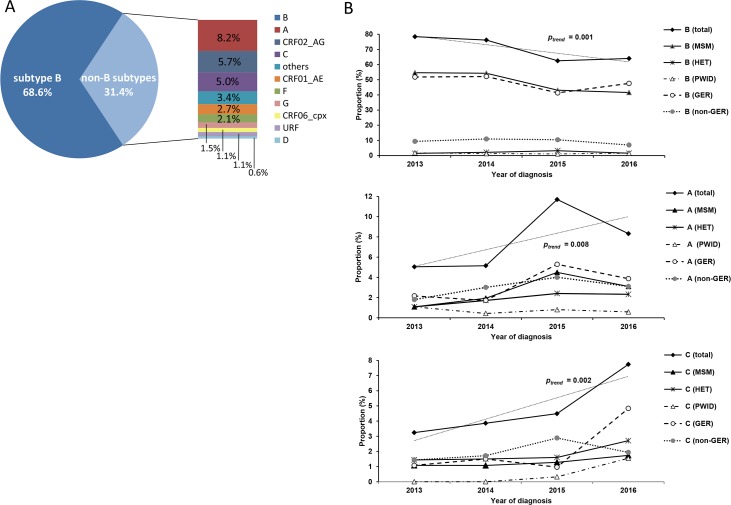
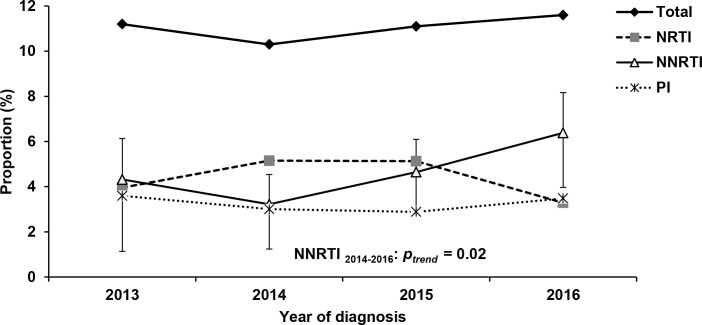
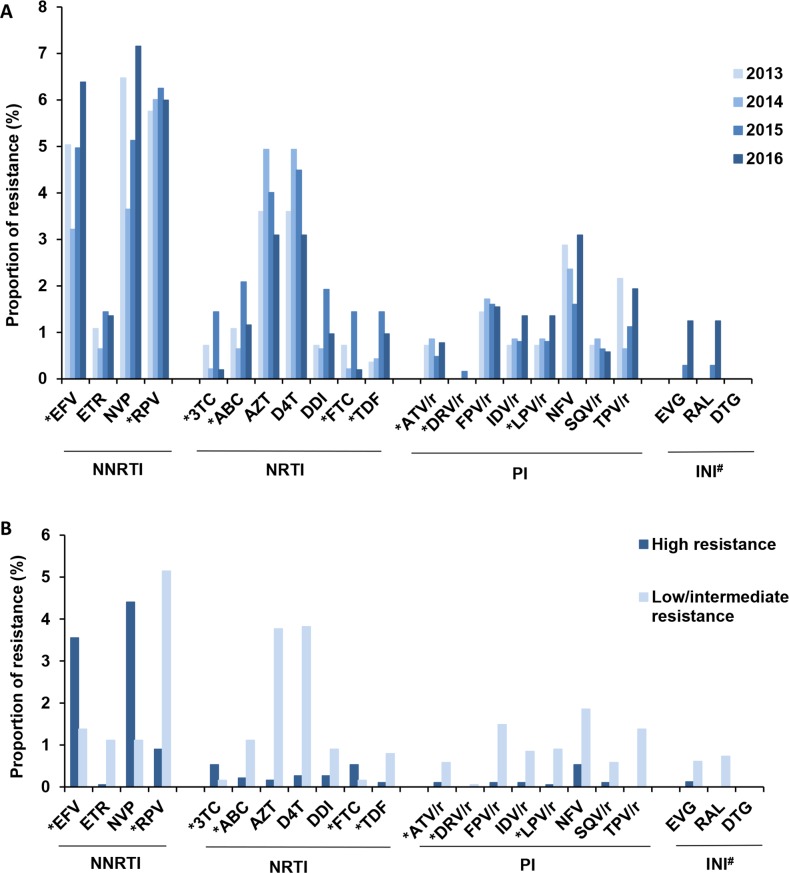
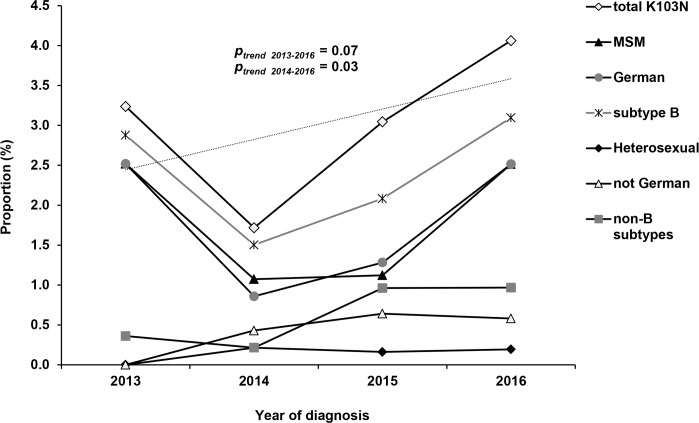
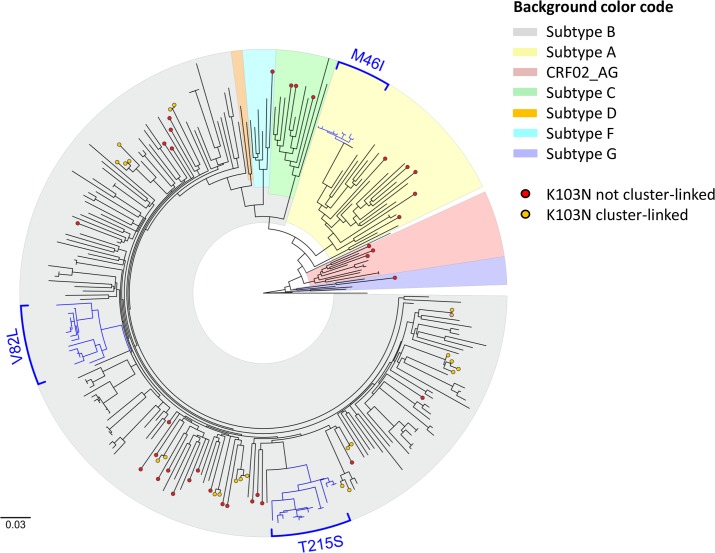
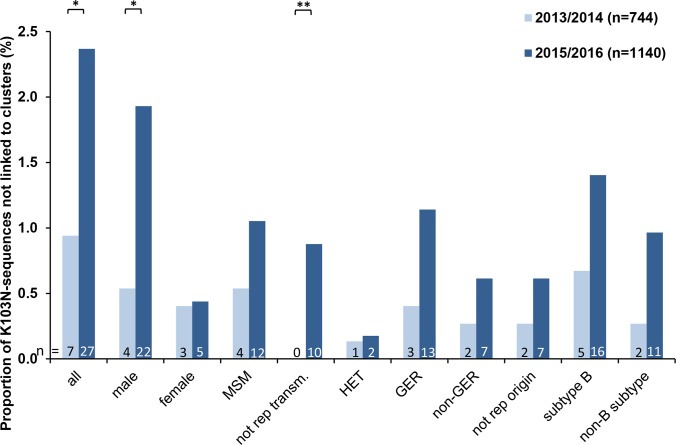
Results: Between January 2013 and December 2016, 1,885 recent infections were analysed regarding the PR/RT genomic region, with 43.5% of these also being subjected to the analysis of INT. The proportion of HIV-1 non-B viruses (31.3%; 591/1,885) increased from 21.6% to 36.0%, particularly the subtypes A (5.0% to 8.3%) and C (3.2% to 7.7%; all ptrends < 0.01). The subtype A increment is mainly due to transmissions within men who have sex with men (MSM) while subtype C transmissions are associated with heterosexuals and people who inject drugs. The prevalence of TDR was stable at 11.0% (208/1,885) over the study period. Resistances to nucleotide RT inhibitors (NRTI) and PR inhibitors (PI) were 4.5% and 3.2%, respectively, without identifiable trends. In contrast, resistances to non-NRTIs (NNRTI, 4.7%) doubled between 2014 and 2016 from 3.2% to 6.4% (ptrend = 0.02) mainly due to the K103N mutation (from 1.7% to 4.1%; ptrend = 0.03) predominantly detected in recently infected German MSM not linked to transmission clusters. Transmitted INSTI mutations were present in only one case (T66I) and resistance to dolutegravir was not identified at all. Reduced susceptibility to recommended first-line therapies was low with 1.0% for PIs, 1.3% for NRTIs and 0.7% for INSTIs, but high for the NNRTIs efavirence (4.9%) and rilpivirine (6.0%) due to the K103N mutation and the polymorphic mutation E138A. These trends in therapy-naïve individuals impact current first-line regimens and require awareness and vigilant surveillance.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- ECDC ECfDPaC. HIV/AIDS surveillance in Europe 2017–2016 data Stockholm: ECDC, 2017.
-
- Wittkop L, Gunthard HF, de Wolf F, Dunn D, Cozzi-Lepri A, de Luca A, et al. Effect of transmitted drug resistance on virological and immunological response to initial combination antiretroviral therapy for HIV (EuroCoord-CHAIN joint project): a European multicohort study. Lancet Infect Dis. 2011;11(5):363–71. 10.1016/S1473-3099(11)70032-9 . - DOI - PubMed
-
- Deutsche AIDS-Gesellschaft (DAIG), Österreichische AIDS-Gesellschaft (ÖAIG), Deutsche Gesellschaft für Innere Medizin (DGIM), Deutsche STI-Gesellschaft (DSTIG), Deutsche Gesellschaft für Infektiologie (DGI), Gesellschaft für Virologie (GfV), et al. Deutsch-Österreichische Leitlinien zur antiretroviralen Therapie der HIV-Infektion. 2015. p. 50.
-
- European AIDS Clinical Society (EACS). Guidelines Version 9.0 October 2017. European Guidelines for treatment of HIV-infected adults in Europe2017.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
