

Resection versus preservation of the middle turbinate in surgery for chronic rhinosinusitis with nasal polyposis: a randomized controlled trial
- PMID: 30409178
- PMCID: PMC6225688
- DOI: 10.1186/s40463-018-0313-8
Resection versus preservation of the middle turbinate in surgery for chronic rhinosinusitis with nasal polyposis: a randomized controlled trial
Abstract
Background: Chronic rhinosinusitis (CRS) affects up to 16% of the population. When medical treatment fails, endoscopic sinus surgery (ESS) is considered. The value of resecting the middle turbinate to optimize surgical outcomes has been hypothesized but remains controversial and unproven. Whether the middle turbinate should be left in place or resected is controversial. Our objective is to determine if middle turbinectomy improves objective surgical outcomes after ESS.
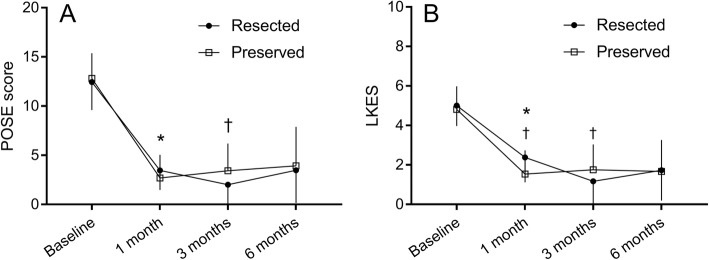
Methods: Sixteen patients (15 men, 15 primary surgery) undergoing bilateral complete ESS for CRS with nasal polyposis were recruited. Nasal cavities were randomized so that middle turbinectomy was performed on one side while the middle turbinate was preserved on the other. Each participant acted as their own control. Nasal cavities were compared using Perioperative Sinus Endoscopy (POSE) and Lund-Kennedy (LKES) scores pre-operatively, and at 1, 3 and 6 months after ESS. Results were analyzed using Wilcoxon signed-rank test.
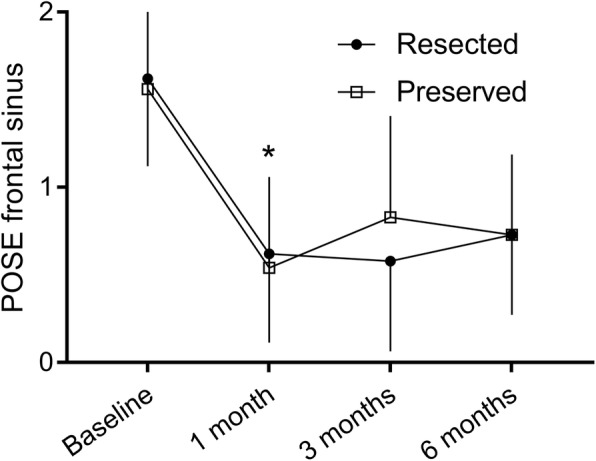
Results: Pre-operatively, the POSE (12.4 ± 2.9 vs 12.8 ± 2.6, p = 0.33, for the preserved side and the resected side, respectively) and LKES (5.0 ± 1.0 vs 4.8 ± 1.2, p = 0.33) scores were similar between sides. During follow up, resection was associated with more crusting at 1 month following ESS (1.0 ± 0.7 vs 0.4 ± 0.6, p = 0.02). There was a small, but statistically significant, difference between the nasal cavities at 3 months, where the resected side showed better endoscopic appearance (2.0 ± 2.2 vs 3.4 ± 2.8, p = 0.01). No difference was found at 6 months. Frontal sinus scores were similar between sides at 6 months (0.7 ± 0.5 vs 0.7 ± 0.5, p = 1.00).
Conclusion: Our results show no sustained objective endoscopic benefit of routine middle turbinectomy, at least within the first six postoperative months, in patients undergoing primary ESS for CRS with polyposis.
Trial registration: NCT, NCT02855931 . Registered 16 August 2016.
Keywords: Chronic rhinosinusitis; Endoscopic sinus surgery; Middle turbinate; Nasal polyposis.
Conflict of interest statement
Ethics approval and consent to participate
Approval was obtained by the Comité d’éthique de la recherche en santé chez l’humain du CIUSSS de l’Estrie – CHUS.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
