An adult autosomal recessive chronic granulomatous disease patient with pulmonary Aspergillus terreus infection
- PMID: 30409207
- PMCID: PMC6225587
- DOI: 10.1186/s12879-018-3451-8
An adult autosomal recessive chronic granulomatous disease patient with pulmonary Aspergillus terreus infection
Abstract
Background: Genetic mutations that reduce intracellular superoxide production by granulocytes causes chronic granulomatous disease (CGD). These patients suffer from frequent and severe bacterial and fungal infections throughout their early life. Diagnosis is usually made in the first 2 years of life but is sometimes only diagnosed when the patient is an adult although they may have suffered from symptoms since childhood.
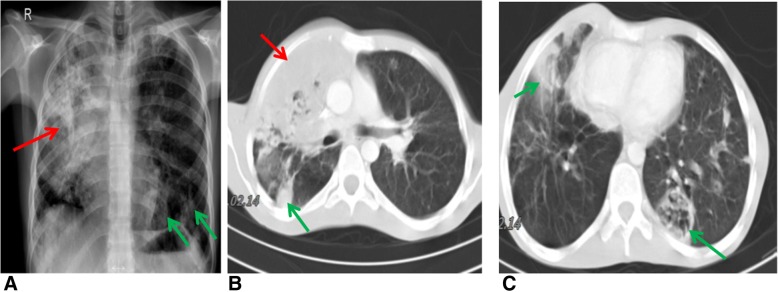
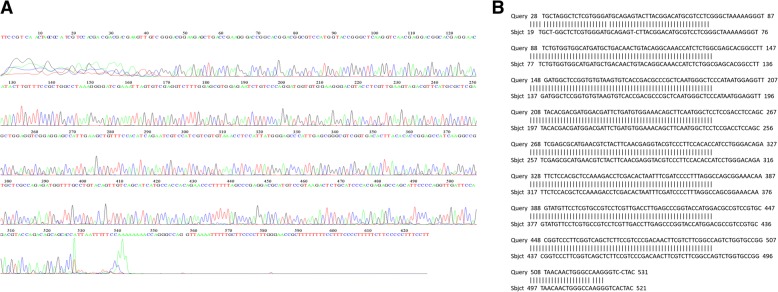
Case presentation: A 26-year-old man was referred with weight loss, fever, hepatosplenomegaly and coughing. He had previously been diagnosed with lymphadenopathy in the neck at age 8 and prescribed anti-tuberculosis treatment. A chest radiograph revealed extensive right-sided consolidation along with smaller foci of consolidation in the left lung. On admission to hospital he had respiratory problems with fever. Laboratory investigations including dihydrorhodamine-123 (DHR) tests and mutational analysis indicated CGD. Stimulation of his isolated peripheral blood neutrophils (PMN) with phorbol 12-myristate 13-acetate (PMA) produced low, subnormal levels of reactive oxygen species (ROS). Aspergillus terreus was isolated from bronchoalveolar lavage (BAL) fluid and sequenced.
Conclusions: We describe, for the first time, the presence of pulmonary A. terreus infection in an adult autosomal CGD patient on long-term corticosteroid treatment. The combination of the molecular characterization of the inherited CGD and the sequencing of fungal DNA has allowed the identification of the disease-causing agent and the optimal treatment to be given as a consequence.
Keywords: Aspergillus terreus; CGD; Pulmonary infection.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Patient consent for case report publication in journal and has signed consent form.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures