

Clostridium difficile infection increases acute and chronic morbidity and mortality
- PMID: 30409240
- PMCID: PMC6624072
- DOI: 10.1017/ice.2018.280
Clostridium difficile infection increases acute and chronic morbidity and mortality
Abstract
Objective: In this study, we aimed to quantify short- and long-term outcomes of Clostridium difficile infection (CDI) in the elderly, including all-cause mortality, transfer to a facility, and hospitalizations.
Design: Retrospective study using 2011 Medicare claims data, including all elderly persons coded for CDI and a sample of uninfected persons. Analysis of propensity score-matched pairs and the entire population stratified by the propensity score was used to determine the risk of all-cause mortality, new transfer to a long-term care facility (LTCF), and short-term skilled nursing facility (SNF), and subsequent hospitalizations within 30, 90, and 365 days.
Results: The claims records of 174,903 patients coded for CDI were compared with those of 1,318,538 control patients. CDI was associated with increased risk of death (odds ratio [OR], 1.77; 95% confidence interval [CI], 1.74-1.81; attributable mortality, 10.9%), new LTCF transfer (OR, 1.74; 95% CI, 1.67-1.82), and new SNF transfer (OR, 2.52; 95% CI, 2.46-2.58) within 30 days in matched-pairs analyses. In a stratified analysis, CDI was associated with greatest risk of 30-day all-cause mortality in persons with lowest baseline probability of CDI (hazard ratio [HR], 3.04; 95% CI, 2.83-3.26); the risk progressively decreased as the baseline probability of CDI increased. CDI was also associated with increased risk of subsequent 30-day, 90-day, and 1-year hospitalization.
Conclusions: CDI was associated with increased risk of short- and long-term adverse outcomes, including transfer to short- and long-term care facilities, hospitalization, and all-cause mortality. The magnitude of mortality risk varied depending on baseline probability of CDI, suggesting that even lower-risk patients may benefit from interventions to prevent CDI.
Conflict of interest statement
D.S. reports no conflicts of interest relevant to this manuscript.
Figures
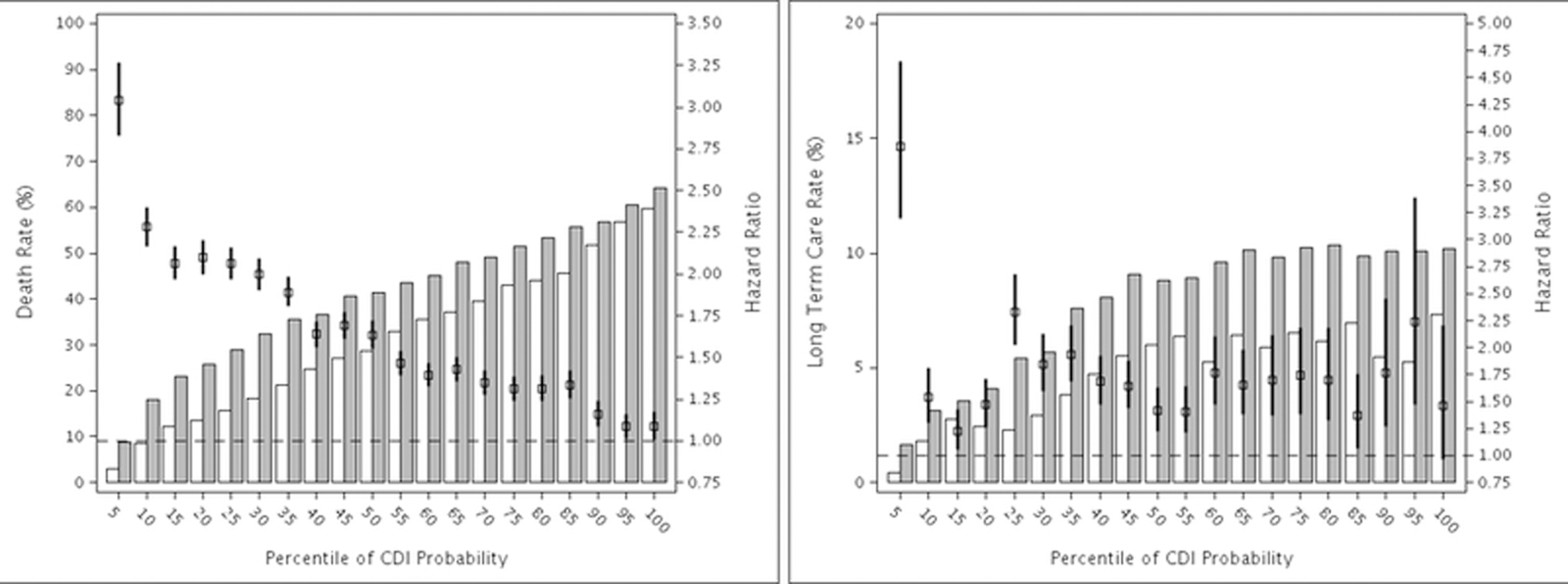
 Hazard ratio and 95% confidence interval.
Hazard ratio and 95% confidence interval.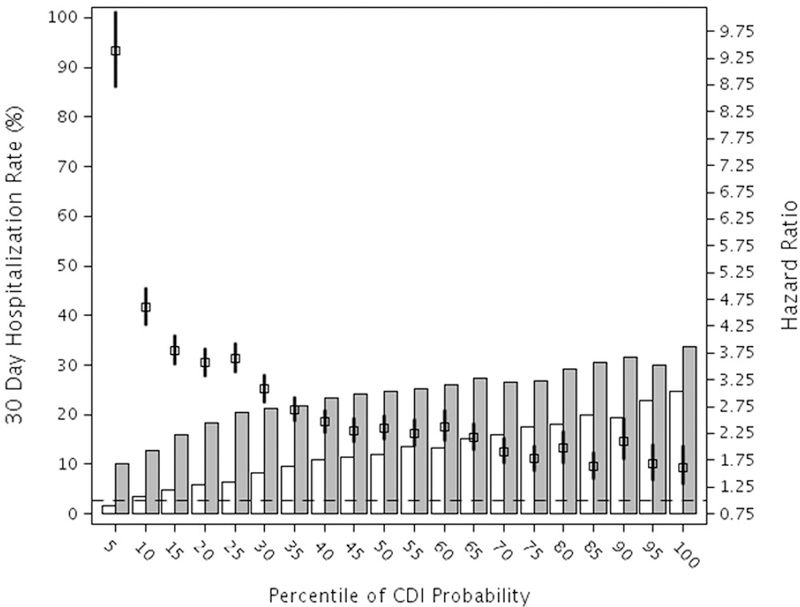
 Hazard ratio and 95% confidence interval. The null hazard ratio of 1.0 is indicated by the horizontal dashed line.
Hazard ratio and 95% confidence interval. The null hazard ratio of 1.0 is indicated by the horizontal dashed line.References
-
- Hall AJ, Curns AT, McDonald LC, Parashar UD, Lopman BA. The roles of Clostridium difficile and norovirus among gastroenteritis-associated deaths in the United States, 1999–2007. Clin Infect Dis 2012;55(2):216–223. - PubMed
-
- Kwon JH, Olsen MA, Dubberke ER. The morbidity, mortality, and costs associated with Clostridium difficile infection. Infect Dis Clin North Am 2015;29(1):123–134. - PubMed
-
- Wiegand PN, Nathwani D, Wilcox MH, Stephens J, Shelbaya A, Haider S. Clinical and economic burden of Clostridium difficile infection in Europe: a systematic review of healthcare-facility-acquired infection. J Hosp Infect 2012;81(1):1–14. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
