

Impact of Statins on Cardiovascular Outcomes Following Coronary Artery Calcium Scoring
- PMID: 30409567
- PMCID: PMC6309473
- DOI: 10.1016/j.jacc.2018.09.051
Impact of Statins on Cardiovascular Outcomes Following Coronary Artery Calcium Scoring
Abstract
Background: Compared with traditional risk factors, coronary artery calcium (CAC) scores improve prognostic accuracy for atherosclerotic cardiovascular disease (ASCVD) outcomes. However, the relative impact of statins on ASCVD outcomes stratified by CAC scores is unknown.
Objectives: The authors sought to determine whether CAC can identify patients most likely to benefit from statin treatment.
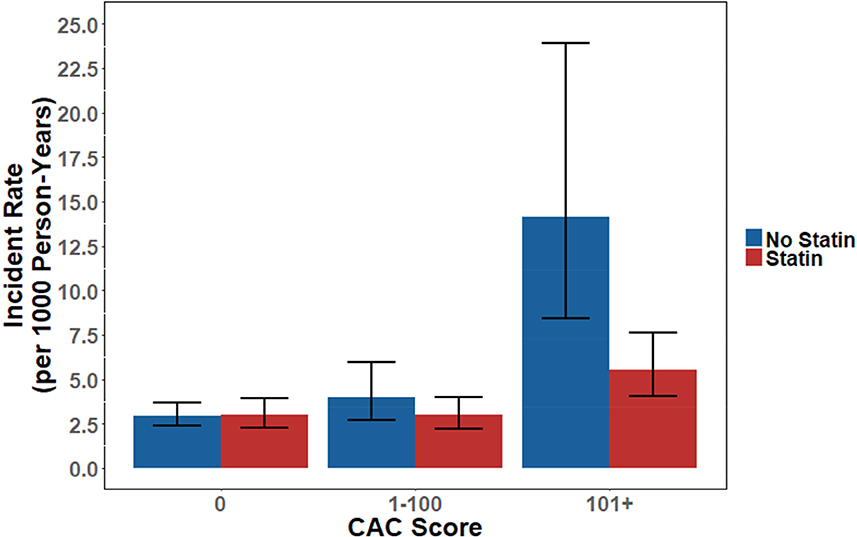
Methods: The authors identified consecutive subjects without pre-existing ASCVD or malignancy who underwent CAC scoring from 2002 to 2009 at Walter Reed Army Medical Center. The primary outcome was first major adverse cardiovascular event (MACE), a composite of acute myocardial infarction, stroke, and cardiovascular death. The effect of statin therapy on outcomes was analyzed stratified by CAC presence and severity, after adjusting for baseline comorbidities with inverse probability of treatment weights based on propensity scores.
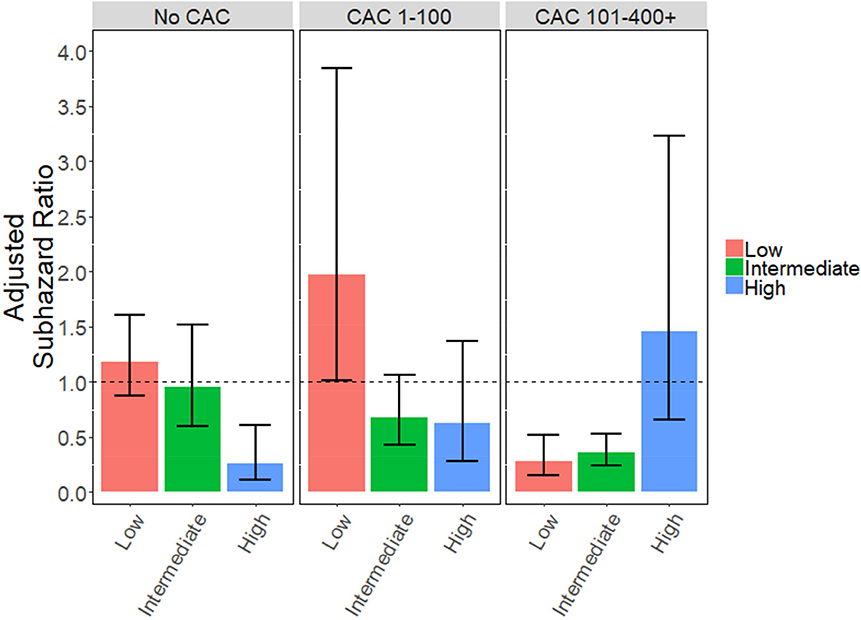
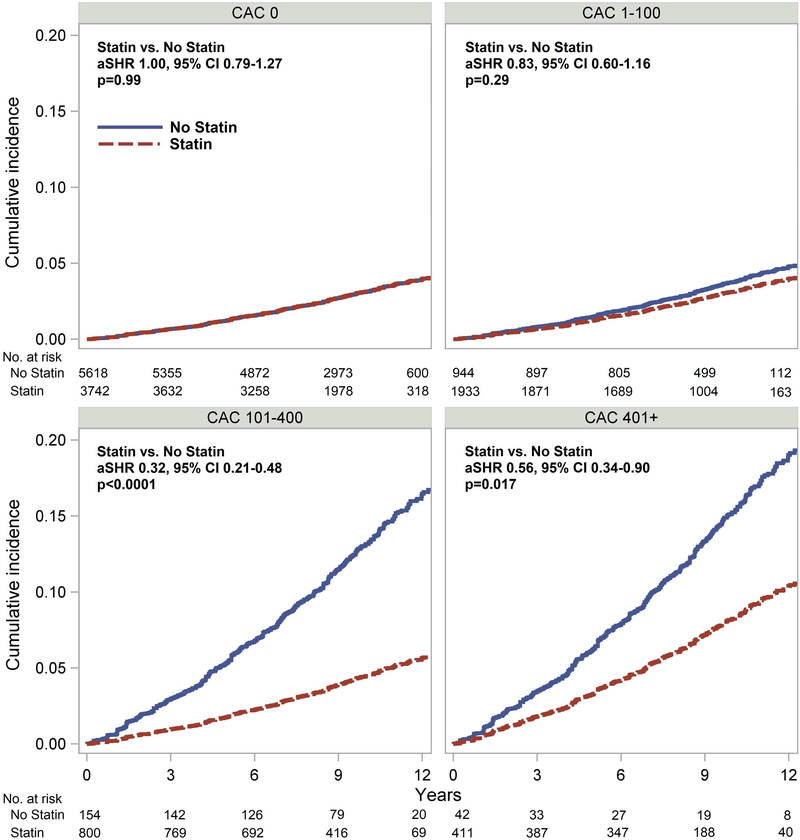
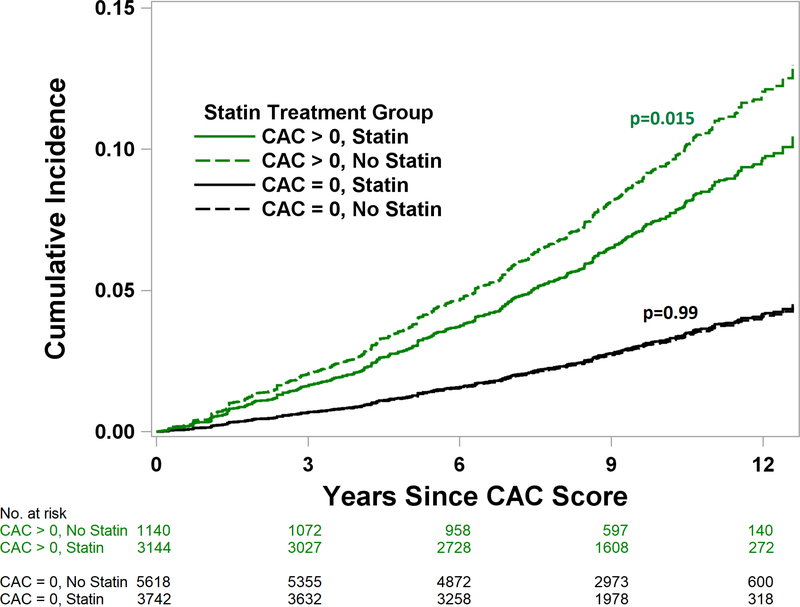
Results: A total of 13,644 patients (mean age 50 years; 71% men) were followed for a median of 9.4 years. Comparing patients with and without statin exposure, statin therapy was associated with reduced risk of MACE in patients with CAC (adjusted subhazard ratio: 0.76; 95% confidence interval: 0.60 to 0.95; p = 0.015), but not in patients without CAC (adjusted subhazard ratio: 1.00; 95% confidence interval: 0.79 to 1.27; p = 0.99). The effect of statin use on MACE was significantly related to the severity of CAC (p < 0.0001 for interaction), with the number needed to treat to prevent 1 initial MACE outcome over 10 years ranging from 100 (CAC 1 to 100) to 12 (CAC >100).
Conclusions: In a largescale cohort without baseline ASCVD, the presence and severity of CAC identified patients most likely to benefit from statins for the primary prevention of cardiovascular diseases.
Keywords: atherosclerotic cardiovascular disease; calcium score; cardiovascular risk; primary prevention; screening.
Copyright © 2018 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Message for 2018 Cholesterol Management Guidelines Update: Time to Accept the Power of Zero.J Am Coll Cardiol. 2018 Dec 25;72(25):3243-3245. doi: 10.1016/j.jacc.2018.10.006. J Am Coll Cardiol. 2018. PMID: 30409568 No abstract available.
-
Reliability of Coronary Artery Calcium Score for Guiding Statin Therapy in Young Individuals.J Am Coll Cardiol. 2019 Apr 16;73(14):1871-1872. doi: 10.1016/j.jacc.2019.01.044. J Am Coll Cardiol. 2019. PMID: 30975307 No abstract available.
-
Confusing Data Analysis.J Am Coll Cardiol. 2019 Apr 16;73(14):1872-1873. doi: 10.1016/j.jacc.2018.11.065. J Am Coll Cardiol. 2019. PMID: 30975308 No abstract available.
-
Reply: Coronary Artery Calcium Screening in the Young and Other Responses: The Walter Reed Cohort.J Am Coll Cardiol. 2019 Apr 16;73(14):1873-1874. doi: 10.1016/j.jacc.2019.02.017. J Am Coll Cardiol. 2019. PMID: 30975309 No abstract available.
-
The Value of Coronary Artery Calcium in Statin-Treated Patients.J Am Coll Cardiol. 2019 Apr 16;73(14):1873. doi: 10.1016/j.jacc.2019.01.046. J Am Coll Cardiol. 2019. PMID: 30975310 No abstract available.
References
References for Online Appendix
-
- Stone NJ, Robinson J, Lichtenstein AH et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2013. - PubMed
-
- Smith MEB, Lee NJ, Haney E, Carson S Drug Class Reviews Drug Class Review: HMG-CoA Reductase Inhibitors (Statins) and Fixed-dose Combination Products Containing a Statin: Final Report Update 5. Portland (OR): Oregon Health & Science University, Portland, Oregon., 2009. - PubMed
-
- Rothman KJ Induction and latent periods. Am J Epidemiol 1981;114:253–9. - PubMed
-
- Nielsen LH, Lokkegaard E, Andreasen AH, Keiding N Using prescription registries to define continuous drug use: how to fill gaps between prescriptions. Pharmacoepidemiol Drug Saf 2008;17:384–8. - PubMed
References
-
- Piepoli MF, Hoes AW, Agewall S et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts): Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J. 2016;37(29):2315–2381. - PMC - PubMed
-
- Stone NJ, Robinson J, Lichtenstein AH et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014;63(25 Pt B):2889–934. - PubMed
-
- Hecht H, Blaha MJ, Berman DS et al. Clinical indications for coronary artery calcium scoring in asymptomatic patients: Expert consensus statement from the Society of Cardiovascular Computed Tomography. J Cardiovasc Comput Tomogr 2017;11:157–168. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
