

Efficacy, Safety, and Biomarkers of Response to Azacitidine and Nivolumab in Relapsed/Refractory Acute Myeloid Leukemia: A Nonrandomized, Open-Label, Phase II Study
- PMID: 30409776
- PMCID: PMC6397669
- DOI: 10.1158/2159-8290.CD-18-0774
Efficacy, Safety, and Biomarkers of Response to Azacitidine and Nivolumab in Relapsed/Refractory Acute Myeloid Leukemia: A Nonrandomized, Open-Label, Phase II Study
Abstract
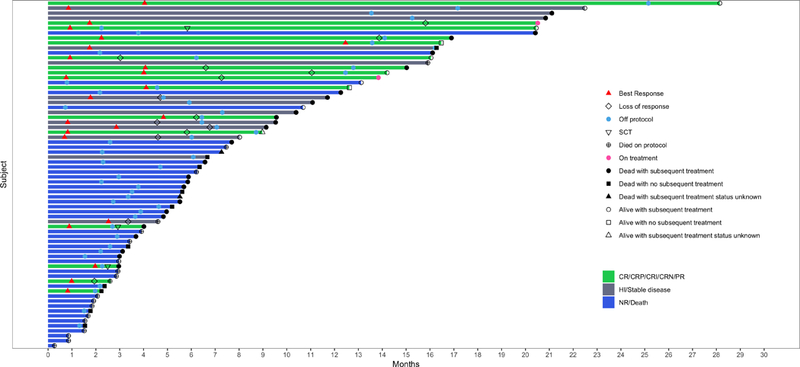
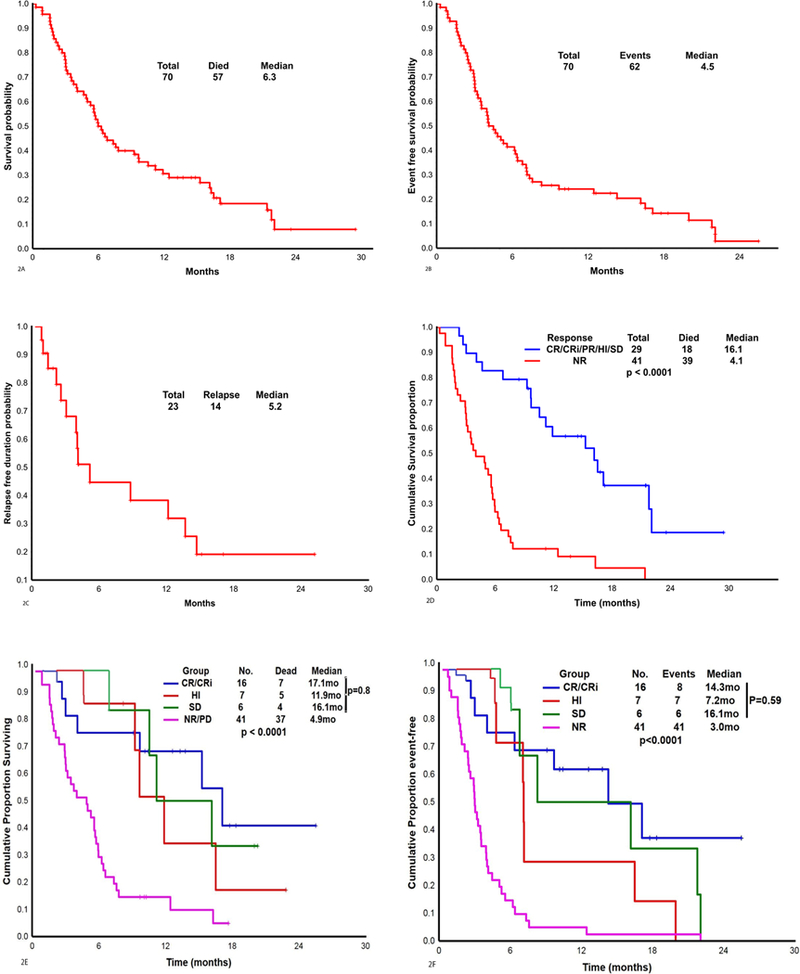
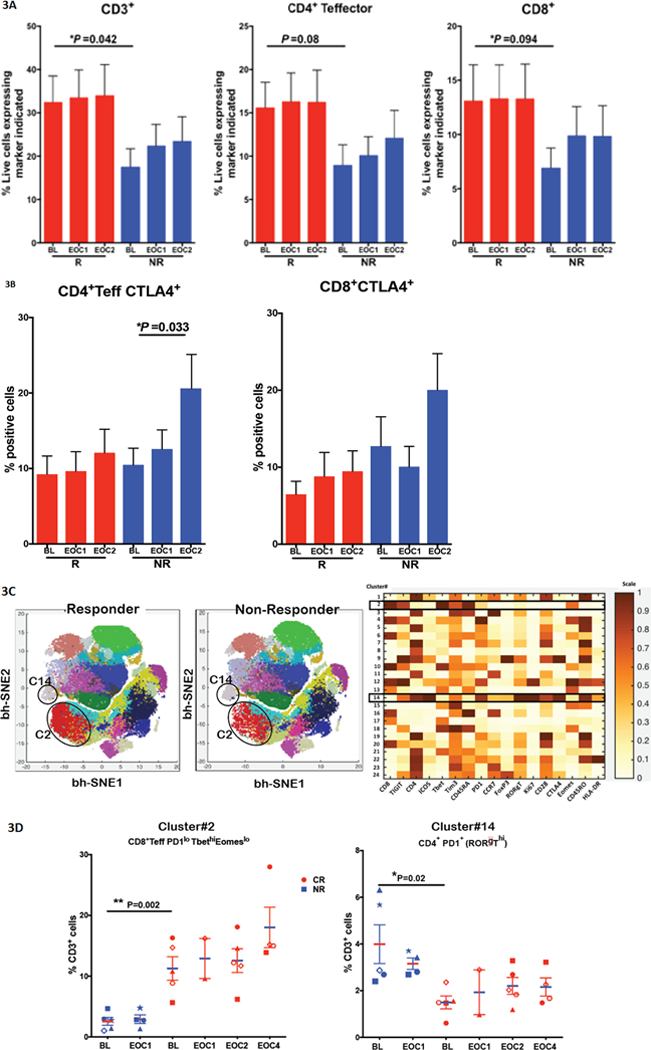
Preclinical models have shown that blocking PD-1/PD-L1 pathways enhances antileukemic responses. Azacitidine upregulates PD-1 and IFNγ signaling. We therefore conducted this single-arm trial, in which patients with relapsed/refractory (R/R) acute myeloid leukemia (AML) were treated with azacitidine 75 mg/m2 days 1 to 7 intravenously or subcutaneously with nivolumab 3 mg/kg intravenously on days 1 and 14, every 4 to 6 weeks. For the seventy patients who were treated, the median age was 70 years (range, 22-90) and the median number of prior therapies received was 2 (range, 1-7). The overall response rate (ORR) was 33%, including 15 (22%) complete remission/complete remission with insufficient recovery of counts, 1 partial response, and 7 patients with hematologic improvement maintained >6 months. Six patients (9%) had stable disease >6 months. The ORR was 58% and 22%, in hypomethylating agent (HMA)-naïve (n = 25) and HMA-pretreated (n = 45) patients, respectively. Grade 3 to 4 immune-related adverse events occurred in 8 (11%) patients. Pretherapy bone marrow and peripheral blood CD3 and CD8 were significantly predictive for response on flow cytometry. CTLA4 was significantly upregulated on CD4+ Teff in nonresponders after 2 and 4 doses of nivolumab. Azacitidine and nivolumab therapy produced an encouraging response rate and overall survival in patients with R/R AML, particularly in HMA-naïve and salvage 1 patients. Pretherapy bone marrow aspirate and peripheral blood CD3 percentage may be biomarkers for patient selection. SIGNIFICANCE: Azacitidine in combination with nivolumab appeared to be a safe and effective therapy in patients with AML who were salvage 1, prior hypomethylator-naïve, or had increased pretherapy CD3+ bone marrow infiltrate by flow cytometry or IHC. Bone marrow CD3 and CD8 are relatively simple assays that should be incorporated to select patients in future trials. This article is highlighted in the In This Issue feature, p. 305.
©2018 American Association for Cancer Research.
Conflict of interest statement
Figures
References
-
- Berger R, Rotem-Yehudar R, Slama G, Landes S, Kneller A, Leiba M, et al. Phase I safety and pharmacokinetic study of CT-011, a humanized antibody interacting with PD-1, in patients with advanced hematologic malignancies. Clin Cancer Res 2008;14(10):3044–51 doi 10.1158/1078-0432.CCR-07-4079. - DOI - PubMed
-
- Westin JR, Chu F, Zhang M, Fayad LE, Kwak LW, Fowler N, et al. Safety and activity of PD1 blockade by pidilizumab in combination with rituximab in patients with relapsed follicular lymphoma: a single group, open-label, phase 2 trial. Lancet Oncol 2014;15(1):69–77 doi 10.1016/S1470-2045(13)70551-5. - DOI - PMC - PubMed
-
- Rifca Le Dieu DCT, Alan G. Ramsay, Richard Mitter, Faridah Miraki-Moud, Rewas Fatah, Lee Abigail M, Andrew Lister T, Gribben John G. Peripheral blood T cells in acute myeloid leukemia (AML) patients at diagnosis have abnormal phenotype and genotype and form defective immune synapses with AML blasts. . Blood 2009;114(18): p. 3909–16(18):3909–16. - PMC - PubMed
-
- Williams P BS G-MG, Cortes JE, Ravandi F, Al-Hamal Zainab, et al. Checkpoint Expression By Acute Myeloid Leukemia (AML) and the Immune Microenvironment Suppresses Adaptive Immunity. American Society of Hematology, December 2017. (abstract) 2017.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
