

Imaging of Surgical Free Flaps in Head and Neck Reconstruction
- PMID: 30409846
- PMCID: PMC7048589
- DOI: 10.3174/ajnr.A5776
Imaging of Surgical Free Flaps in Head and Neck Reconstruction
Abstract
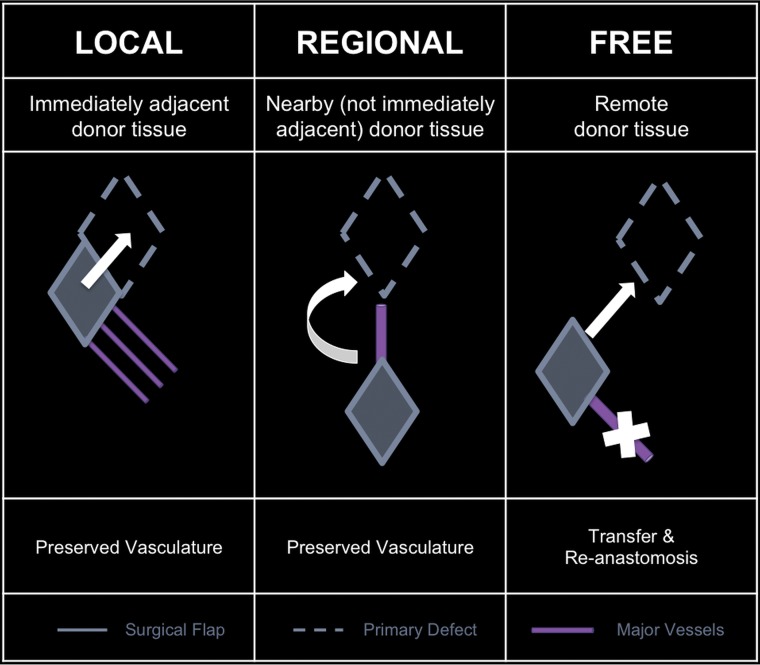
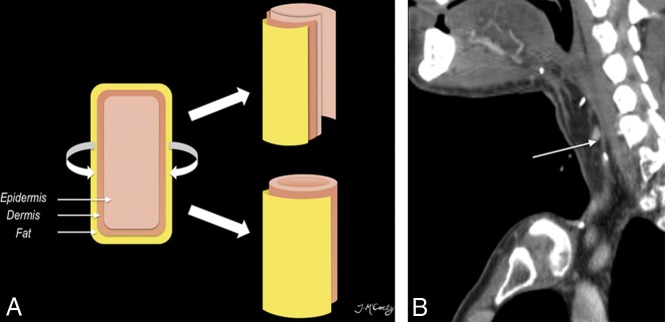
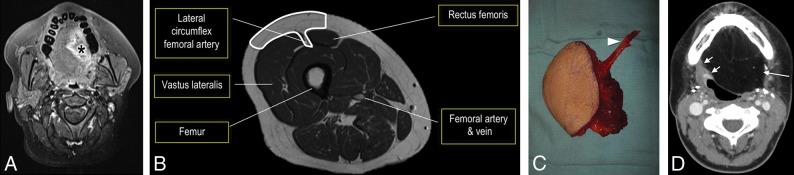
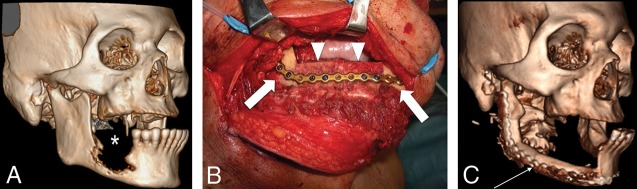
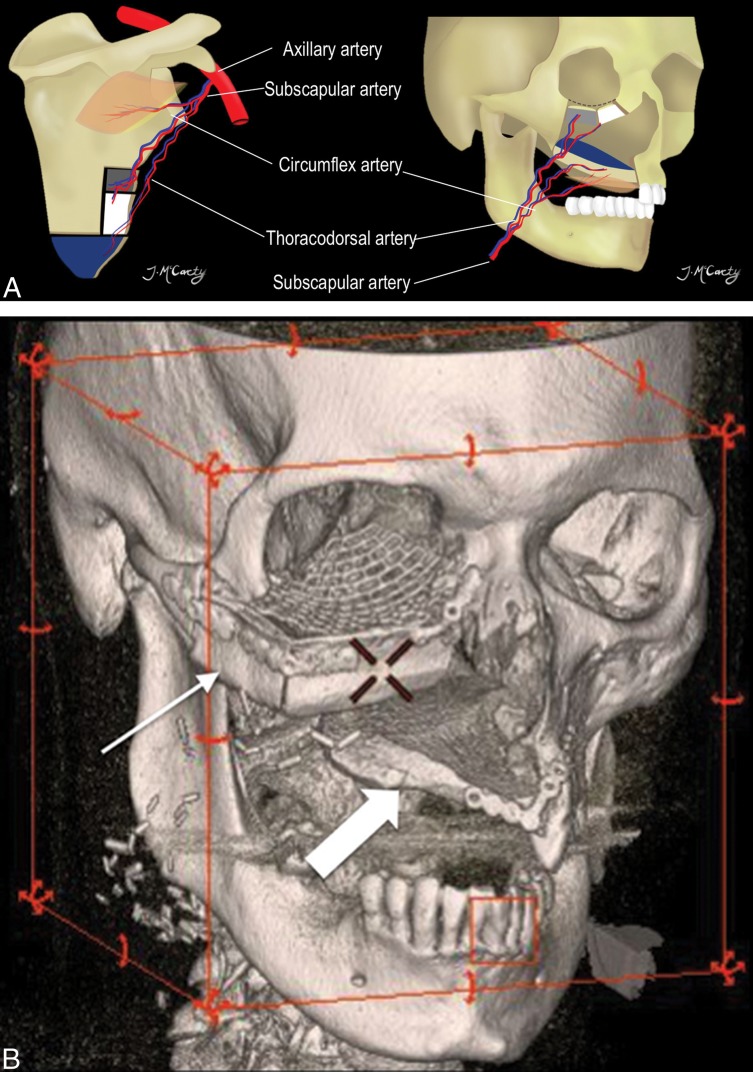
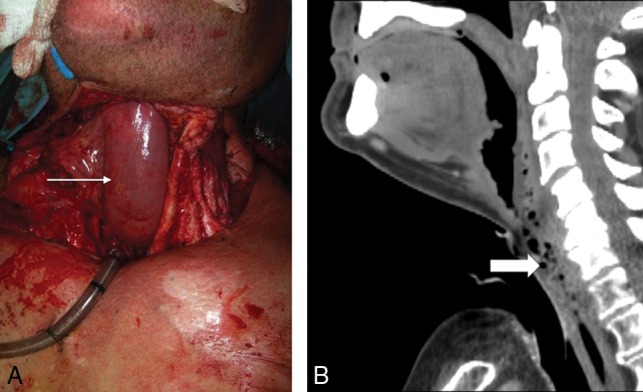
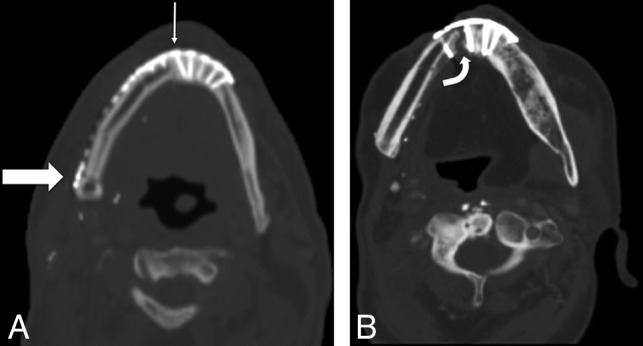
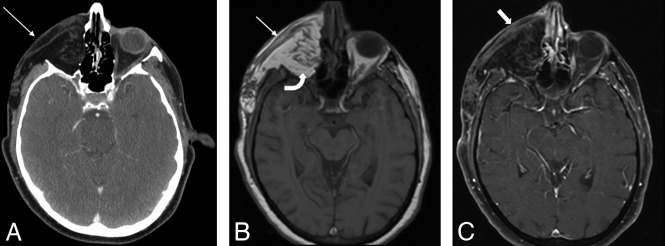
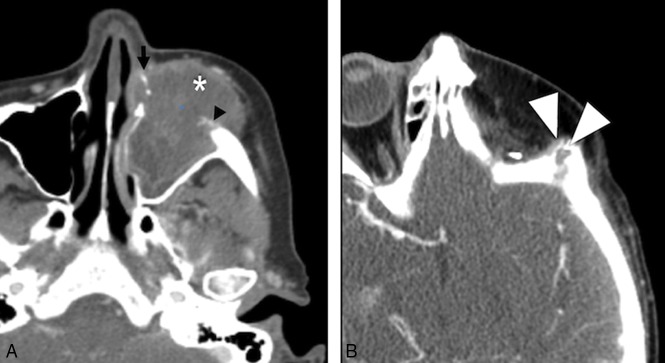
Head and neck surgical reconstruction is complex, and postoperative imaging interpretation is challenging. Surgeons now use microvascular free tissue transfer, also known as free flaps, more frequently in head and neck reconstruction than ever before. Thus, an understanding of free flaps, their expected appearance on cross-sectional imaging, and their associated complications (including tumor recurrence) is crucial for the interpreting radiologist. Despite the complexity and increasing frequency of free flap reconstruction, there is no comprehensive head and neck resource intended for the radiologist. We hope that this image-rich review will fill that void and serve as a go to reference for radiologists interpreting imaging of surgical free flaps in head and neck reconstruction.
© 2019 by American Journal of Neuroradiology.
Figures
References
-
- Urken ML. Atlas of Regional and Free Flaps for Head and Neck Reconstruction. New York: Raven Press; 1995
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical