

Are inequalities in cancer diagnosis through emergency presentation narrowing, widening or remaining unchanged? Longitudinal analysis of English population-based data 2006-2013
- PMID: 30409920
- PMCID: PMC6839789
- DOI: 10.1136/jech-2017-210371
Are inequalities in cancer diagnosis through emergency presentation narrowing, widening or remaining unchanged? Longitudinal analysis of English population-based data 2006-2013
Abstract
Background: Diagnosis of cancer through emergency presentation is associated with poorer prognosis. While reductions in emergency presentations have been described, whether known sociodemographic inequalities are changing is uncertain.
Methods: We analysed 'Routes to Diagnosis' data on patients aged ≥25 years diagnosed in England during 2006-2013 with any of 33 common or rarer cancers. Using binary logistic regression we determined time-trends in diagnosis through emergency presentation by age, deprivation and cancer site.
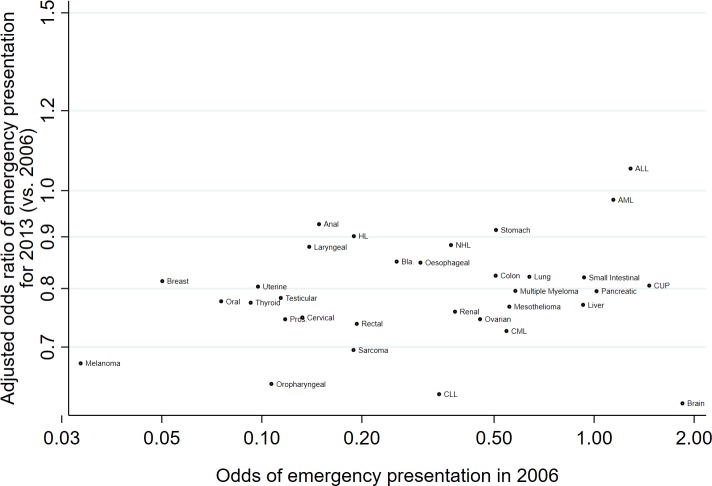
Results: Overall adjusted proportions of emergency presentations decreased during the study period (2006: 23%, 2013: 20%). Substantial baseline (2006) inequalities in emergency presentation risk by age and deprivation remained largely unchanged. There was evidence (p<0.05) of reductions in the risk of emergency presentations for most (28/33) cancer sites, without apparent associations between the size of reduction and baseline risk (p=0.26). If there had been modest reductions in age inequalities (ie, patients in each age group acquiring the same percentage of emergency presentations as the adjacent group with lower risk), in the last study year we could have expected around 11 000 fewer diagnoses through emergency presentation (ie, a nationwide percentage of 16% rather than the observed 20%). For similarly modest reductions in deprivation inequalities, we could have expected around 3000 fewer (ie, 19%).
Conclusion: The proportion of cancer diagnoses through emergency presentation is decreasing but age and deprivation inequalities prevail, indicating untapped opportunities for further improvements by reducing these inequalities. The observed reductions in proportions across nearly all cancer sites are likely to reflect both earlier help-seeking and improvements in diagnostic healthcare pathways, across both easier-to-suspect and harder-to-suspect cancers.
Keywords: ageing; cancer; deprivation; inequalities.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures



References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources