

Streptococcus pneumoniae outbreaks and implications for transmission and control: a systematic review
- PMID: 30410854
- PMCID: PMC6217781
- DOI: 10.1186/s41479-018-0055-4
Streptococcus pneumoniae outbreaks and implications for transmission and control: a systematic review
Abstract
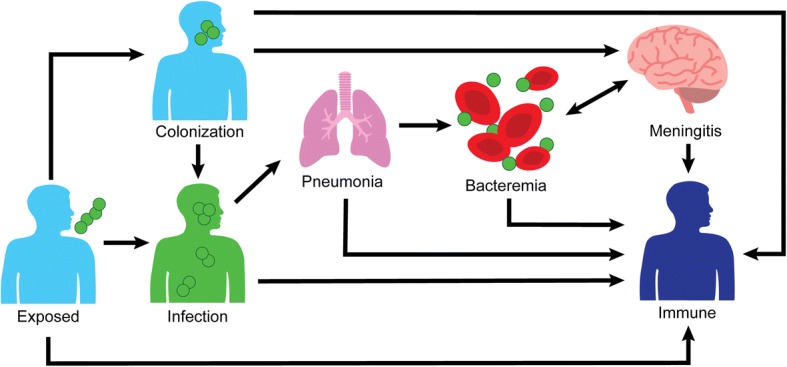
Background: Streptococcus pneumoniae is capable of causing multiple infectious syndromes and occasionally causes outbreaks. The objective of this review is to update prior outbreak reviews, identify control measures, and comment on transmission.
Methods: We conducted a review of published S. pneumoniae outbreaks, defined as at least two linked cases of S. pneumoniae.
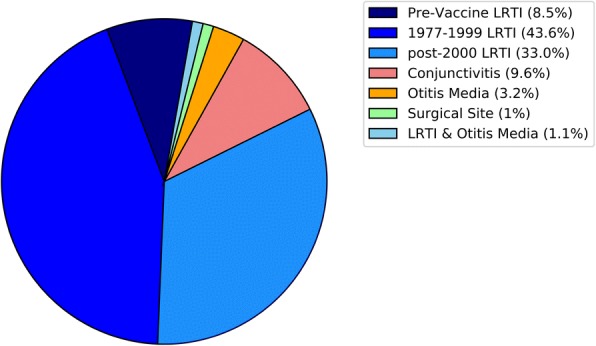
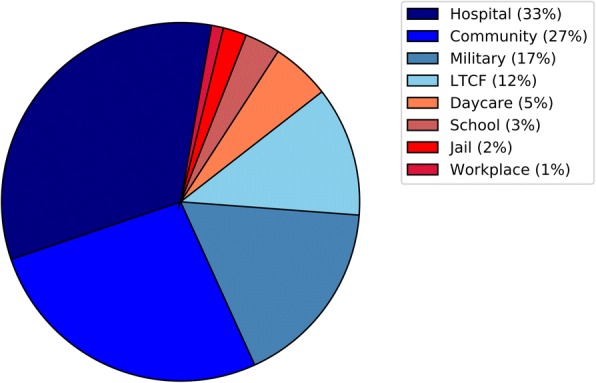
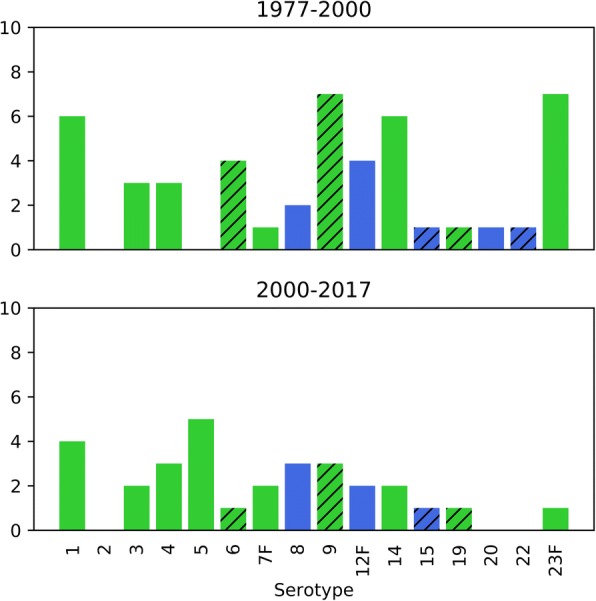
Results: A total of 98 articles (86 respiratory; 8 conjunctivitis; 2 otitis media; 1 surgical site; 1 multiple), detailing 94 unique outbreaks occurring between 1916 to 2017 were identified. Reported serotypes included 1, 2, 3, 4, 5, 7F, 8, 12F, 14, 20, and 23F, and serogroups 6, 9, 15, 19, 22. The median attack rate for pneumococcal outbreaks was 7.0% (Interquartile range: 2.4%, 13%). The median case-fatality ratio was 12.9% (interquartile range: 0%, 29.2%). Age groups most affected by outbreaks were older adults (60.3%) and young adults (34.2%). Outbreaks occurred in crowded settings, such as universities/schools/daycares, military barracks, hospital wards, and long-term care facilities. Of outbreaks that assessed vaccination coverage, low initial vaccination or revaccination coverage was common. Most (73.1%) of reported outbreaks reported non-susceptibility to at least one antibiotic, with non-susceptibility to penicillin (56.0%) and erythromycin (52.6%) being common. Evidence suggests transmission in outbreaks can occur through multiple modes, including carriers, infected individuals, or medical devices. Several cases developed disease shortly after exposure (< 72 h). Respiratory outbreaks used infection prevention (55.6%), prophylactic vaccination (63.5%), and prophylactic antibiotics (50.5%) to prevent future cases. PPSV23 covered all reported outbreak serotypes. PCV13 covered 10 of 16 serotypes. For conjunctival outbreaks, only infection prevention strategies were used.
Conclusions: To prevent the initial occurrence of respiratory outbreaks, vaccination and revaccination is likely the best preventive measure. Once an outbreak occurs, vaccination and infection-prevention strategies should be utilized. Antibiotic prophylaxis may be considered for high-risk exposed individuals, but development of antibiotic resistance during outbreaks has been reported. The short period between initial exposure and development of disease indicates that pneumococcal colonization is not a prerequisite for pneumococcal respiratory infection.
Keywords: Cluster; Epidemic; Outbreaks; Pneumococcal vaccine; Pneumococcus; Streptococcus pneumoniae; Transmission.
Conflict of interest statement
Not applicable.Not applicable.JDG is an employee of Merck & Co., Inc. SIB-D received investigator-initiated research funding and served as a consultant for Pfizer. DJW consults for Merck & Co., Inc. and Pfizer Inc., and received payment as part of Merck’s Speaker’s Bureau.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Torres A, Blasi F, Dartois N, Akova M. Which individuals are at increased risk of pneumococcal disease and why? Impact of COPD, asthma, smoking, diabetes, and/or chronic heart disease on community-acquired pneumonia and invasive pneumococcal disease. Thorax. 2015;70:984–989. doi: 10.1136/thoraxjnl-2015-206780. - DOI - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
