

Mean arterial pressure and mortality in patients with distributive shock: a retrospective analysis of the MIMIC-III database
- PMID: 30411243
- PMCID: PMC6223403
- DOI: 10.1186/s13613-018-0448-9
Mean arterial pressure and mortality in patients with distributive shock: a retrospective analysis of the MIMIC-III database
Abstract
Background: Maintenance of mean arterial pressure (MAP) at levels sufficient to avoid tissue hypoperfusion is a key tenet in the management of distributive shock. We hypothesized that patients with distributive shock sometimes have a MAP below that typically recommended and that such hypotension is associated with increased mortality.
Methods: In this retrospective analysis of the Medical Information Mart for Intensive Care (MIMIC-III) database from Beth Israel Deaconess Medical Center, Boston, USA, we included all intensive care unit (ICU) admissions between 2001 and 2012 with distributive shock, defined as continuous vasopressor support for ≥ 6 h and no evidence of low cardiac output shock. Hypotension was evaluated using five MAP thresholds: 80, 75, 65, 60 and 55 mmHg. We evaluated the longest continuous episode below each threshold during vasopressor therapy. The primary outcome was ICU mortality.
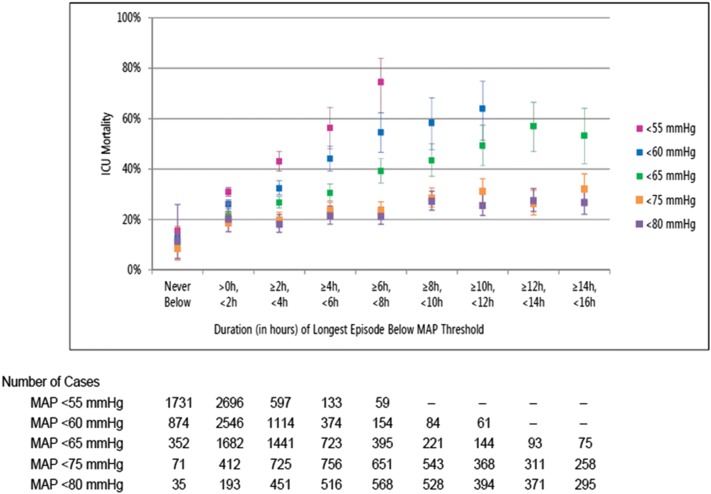
Results: Of 5347 patients with distributive shock, 95.7%, 91.0%, 62.0%, 36.0% and 17.2%, respectively, had MAP < 80, < 75, < 65, < 60 and < 55 mmHg for more than two consecutive hours. On average, ICU mortality increased by 1.3, 1.8, 5.1, 7.9 and 14.4 percentage points for each additional 2 h with MAP < 80, < 75, < 65, < 60 and < 55 mmHg, respectively. Multivariable logistic modeling showed that, compared to patients in whom MAP was never < 65 mmHg, ICU mortality increased as duration of hypotension < 65 mmHg increased [for > 0 to < 2 h, odds ratio (OR) 1.76, p = 0.005; ≥ 6 to < 8 h, OR 2.90, p < 0.0001; ≥ 20 h, OR 7.10, p < 0.0001]. When hypotension was defined as MAP < 60 or < 55 mmHg, the associations between duration and mortality were generally stronger than when hypotension was defined as MAP < 65 mmHg. There was no association between hypotension and mortality when hypotension was defined as MAP < 80 mmHg.
Conclusions: Within the limitations due to the nature of the study, most patients with distributive shock experienced at least one episode with MAP < 65 mmHg lasting > 2 h. Episodes of prolonged hypotension were associated with higher mortality.
Keywords: Acute circulatory failure; ICU mortality; Mean arterial pressure; Multiple organ failure.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
