

Opposite acute potassium and sodium shifts during transplantation of hypothermic machine perfused donor livers
- PMID: 30411502
- PMCID: PMC6587472
- DOI: 10.1111/ajt.15173
Opposite acute potassium and sodium shifts during transplantation of hypothermic machine perfused donor livers
Abstract
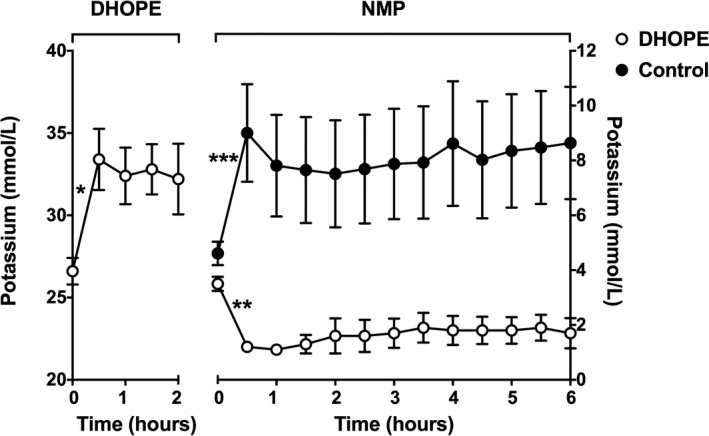
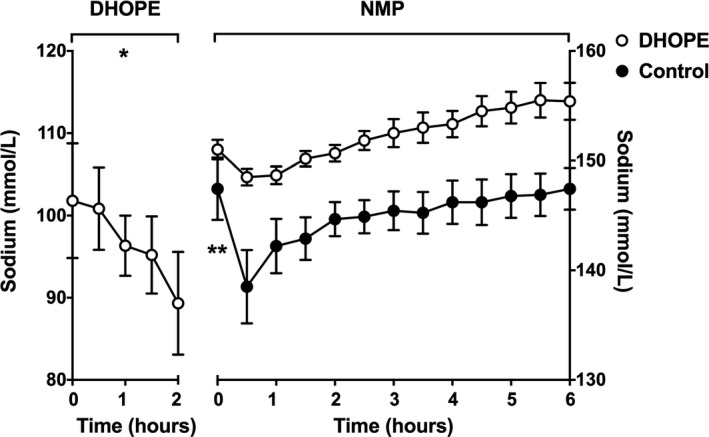
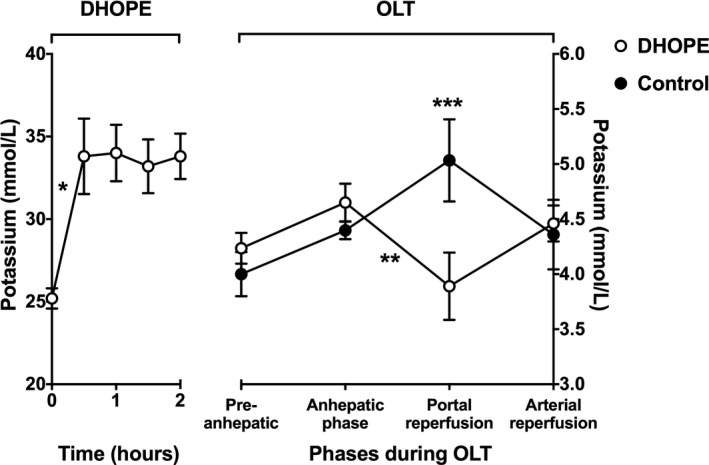
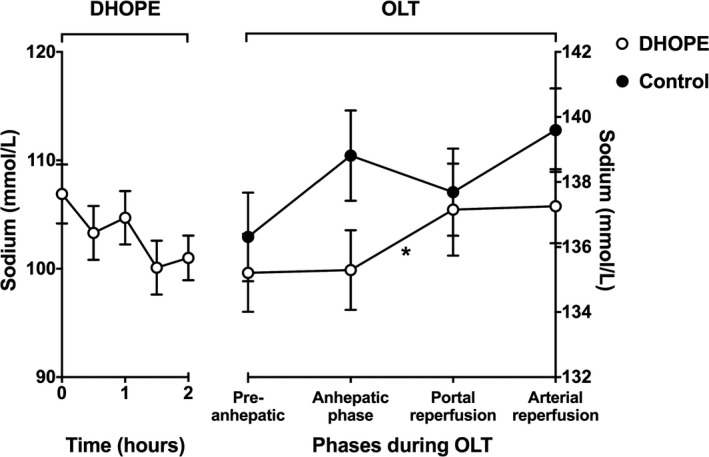
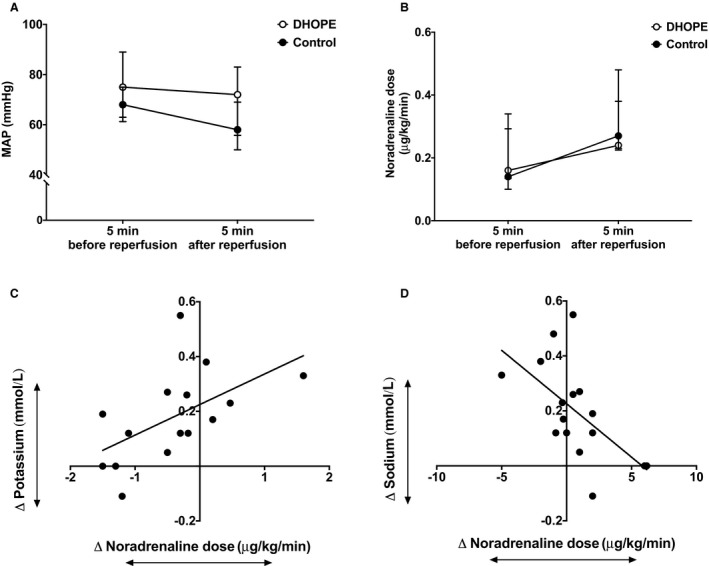
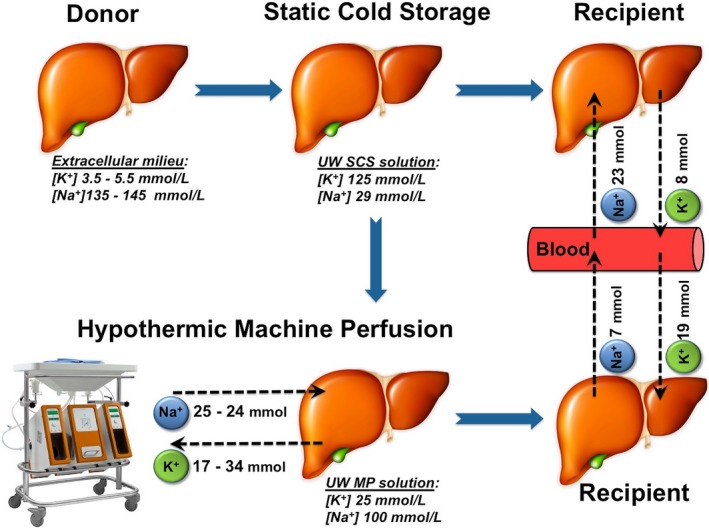
Liver transplantation is frequently associated with hyperkalemia, especially after graft reperfusion. Dual hypothermic oxygenated machine perfusion (DHOPE) reduces ischemia/reperfusion injury and improves graft function, compared to conventional static cold storage (SCS). We examined the effect of DHOPE on ex situ and in vivo shifts of potassium and sodium. Potassium and sodium shifts were derived from balance measurements in a preclinical study of livers that underwent DHOPE (n = 6) or SCS alone (n = 9), followed by ex situ normothermic reperfusion. Similar measurements were performed in a clinical study of DHOPE-preserved livers (n = 10) and control livers that were transplanted after SCS only (n = 9). During DHOPE, preclinical and clinical livers released a mean of 17 ± 2 and 34 ± 6 mmol potassium and took up 25 ± 9 and 24 ± 14 mmol sodium, respectively. After subsequent normothermic reperfusion, DHOPE-preserved livers took up a mean of 19 ± 3 mmol potassium, while controls released 8 ± 5 mmol potassium. During liver transplantation, blood potassium levels decreased upon reperfusion of DHOPE-preserved livers while levels increased after reperfusion of SCS-preserved liver, delta potassium levels were -0.77 ± 0.20 vs. +0.64 ± 0.37 mmol/L, respectively (P = .002). While hyperkalemia is generally anticipated during transplantation of SCS-preserved livers, reperfusion of hypothermic machine perfused livers can lead to decreased blood potassium or even hypokalemia in the recipient.
Keywords: donors and donation; liver transplantation/hepatology; organ perfusion and preservation; translational research/science.
© 2018 The Authors. American Journal of Transplantation published by Wiley Periodicals, Inc. on behalf of The American Society of Transplantation and the American Society of Transplant Surgeons.
Figures
Comment in
-
Postreperfusion syndrome, hyperkalemia and machine perfusion in liver transplantation.Transl Gastroenterol Hepatol. 2019 Sep 11;4:68. doi: 10.21037/tgh.2019.08.12. eCollection 2019. Transl Gastroenterol Hepatol. 2019. PMID: 31620650 Free PMC article. No abstract available.
References
-
- Nakasuji M, Bookallil MJ. Pathophysiological mechanisms of postrevascularization hyperkalemia in orthotopic liver transplantation. Anesth Analg. 2000;91(6):1351‐1355. - PubMed
-
- Xia VW, Ghobrial RM, Du B, et al. Predictors of hyperkalemia in the prereperfusion, early postreperfusion, and late postreperfusion periods during adult liver transplantation. Anesth Analg. 2007;105(3):780‐785. - PubMed
-
- Chen J, Singhapricha T, Memarzadeh M, et al. Storage age of transfused red blood cells during liver transplantation and its intraoperative and postoperative effects. World J Surg. 2012;36(10):2436‐2442. - PubMed
-
- Carmicheal FJ, Lindop MJ, Farman JV. Anesthesia for hepatic transplantation: cardiovascular and metabolic alterations and their management. Anesth Analg. 1985;64(2):108‐116. - PubMed
-
- Acosta F, Sansano T, Contreras RF, et al. Changes in serum potassium during reperfusion in liver transplantation. Transplant Proc. 1999;31(6):2382‐2383. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
