

Update on Chronic Kidney Disease Mineral and Bone Disorder in Cardiovascular Disease
- PMID: 30413250
- PMCID: PMC6372293
- DOI: 10.1016/j.semnephrol.2018.08.001
Update on Chronic Kidney Disease Mineral and Bone Disorder in Cardiovascular Disease
Abstract
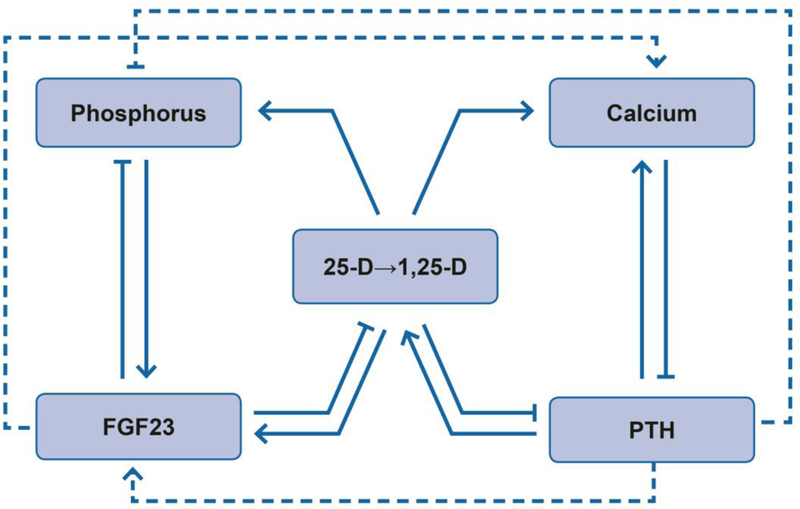
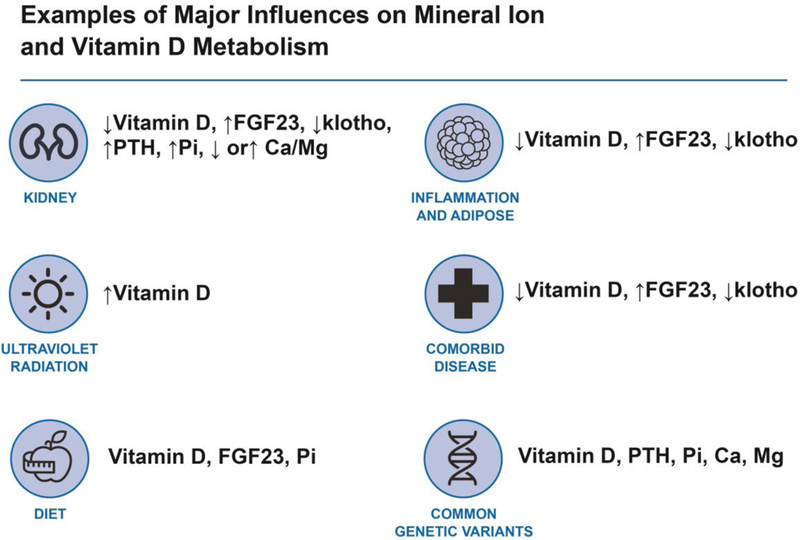
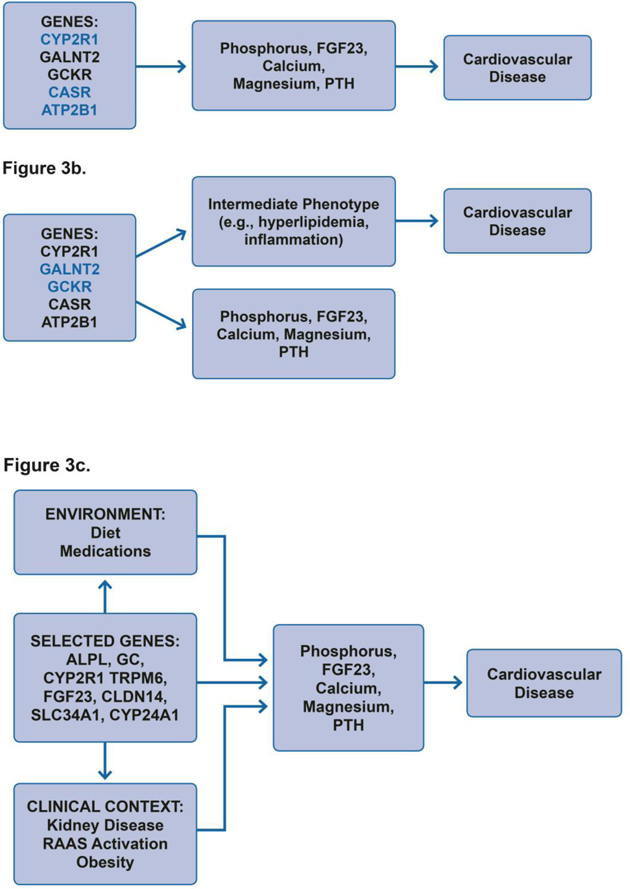
Chronic kidney disease mineral and bone disorder (MBD) encompasses changes in mineral ion and vitamin D metabolism that are widespread in the setting of chronic kidney disease and end-stage renal disease. MBD components associate with cardiovascular disease in many epidemiologic studies. Through impacts on hypertension, activation of the renin-angiotensin-aldosterone system, vascular calcification, endothelial function, and cardiac remodeling and conduction, MBD may be a direct and targetable cause of cardiovascular disease. However, assessment and treatment of MBD is rife with challenges owing to biological tensions between its many components, such as calcium and phosphorus with their regulatory hormones fibroblast growth factor 23 and parathyroid hormone; fibroblast growth factor 23 with its co-receptor klotho; and vitamin D with control of calcium and phosphorus. These complex interactions between MBD components hinder the simple translation to clinical trials, which ultimately are needed to prove the benefits of treating MBD. Deeper investigation using precision medicine tools and principles, including genomics and individualized risk assessment and therapy, may help move the field closer toward clinical applications. This review provides a high-level overview of conventional and precision epidemiology in MBD, potential mechanisms of cardiovascular disease pathogenesis, and guiding therapeutic principles for established and emerging treatments.
Keywords: Cardiovascular disease; fibroblast growth factor 23; klotho; mineral metabolism; phosphorus; vitamin D.
Published by Elsevier Inc.
Figures
References
-
- Kidney Disease: Improving Global Outcomes (KDIGO) Chronic Kidney Disease Mineral and Bone Disorder Working Group. KDIGO 2017 clinical practice guideline update for the diagnosis, evaluation, prevention, and treatment of chronic kidney disease–mineral and bone disorder (CKD-MBD). Kidney Int Suppl 2017;7:1–59. - PMC - PubMed
-
- Isakova T, Wahl P, Vargas GS, Gutierrez OM, Scialla J, Xie H, Appleby D, Nessel L, Bellovich K, Chen J, Hamm L, Gadegbeku C, Horwitz E, Townsend RR, Anderson CA, Lash JP, Hsu CY, Leonard MB, Wolf M. Fibroblast growth factor 23 is elevated before parathyroid hormone and phosphate in chronic kidney disease. Kidney Int 2011;79(12):1370–1378. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
