

Systematic review of single-incision versus conventional multiport laparoscopic surgery for sigmoid colon and rectal cancer
- PMID: 30414613
- PMCID: PMC6230377
- DOI: 10.1186/s12957-018-1521-4
Systematic review of single-incision versus conventional multiport laparoscopic surgery for sigmoid colon and rectal cancer
Abstract
Objectives: To explore whether single-incision laparoscopic surgery (SILS) has the better short-term clinical and pathological outcomes than conventional multiport laparoscopic surgery (CLS) for sigmoid colon and rectal cancer.
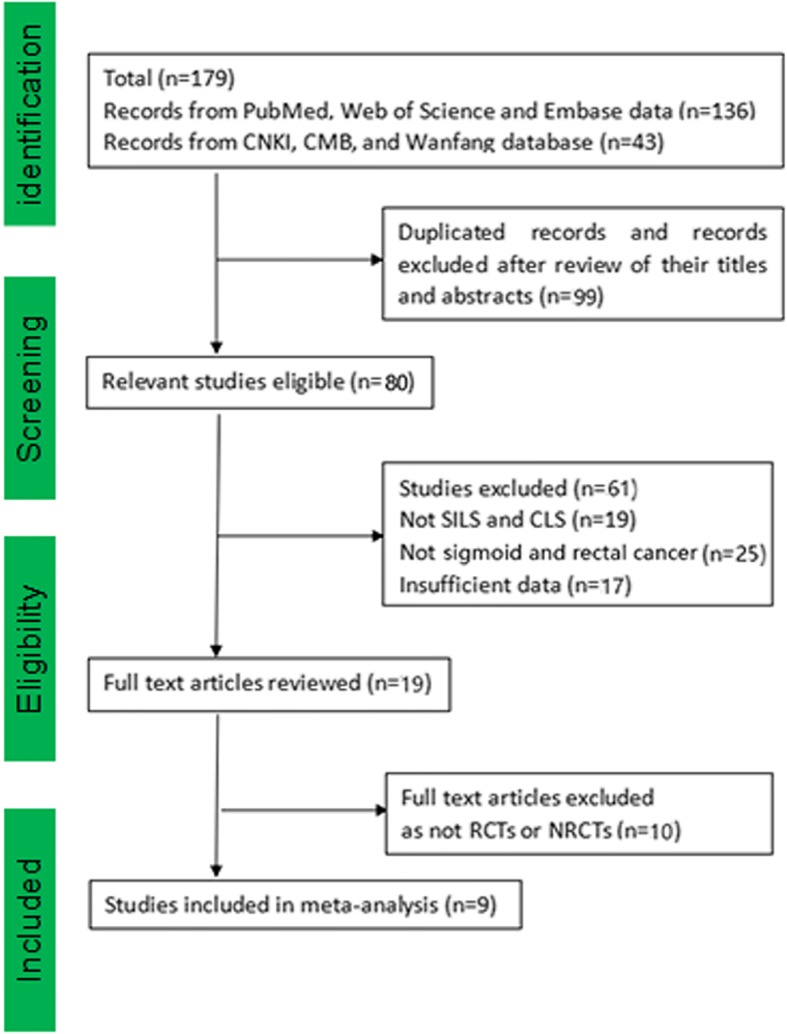
Methods: A literature investigation of MEDLINE, PubMed, Ovid, Embase, Cochrane Library, Web of Science, Chinese National Knowledge Infrastructure (CNKI), Chinese Biological Medicine (CBM), and Wanfang databases for relevant researches was performed. Fixed effects and random effects models were used to calculate the corresponding outcomes. Standardized mean difference and risk ratio were calculated for continuous and dichotomous variables separately.
Results: Nine clinical controlled trials were composed of two randomized clinical trials and seven non-randomized clinical trials with a total of 829 patients. Two hundred ninety-nine (36.1%) patients underwent SILS, and 530 (63.9%) patients underwent CLS. The meta-analysis showed that SILS had more lymph node resection (SMD - 0.25, 95% CI - 0.50 to - 0.002) and less defecation time (SMD - 0.46, 95% CI - 0.75 to - 0.17), exhaust time (SMD - 0.46, 95% CI - 0.75 to - 0.18), and hospital stay (SMD - 0.30, 95% CI - 0.45 to - 0.15 than CLS. SILS was also accompanied with shorter incision length (SMD - 2.46, 95% CI - 4.02 to - 0.90), less pain score (SMD - 0.56, 95% CI - 0.91 to - 0.21), and lower complication rate (RR 0.66, 95% CI 0.47 to 0.91). Blood loss, operative time, distal margin, conversion rate, anastomotic fistula, readmission, local recurrence, and distant metastasis showed no statistical differences in two groups. In all subgroup analysis, SILS also had advantages of incision length, operative time, defecation time, exhaust time, and hospitalization time than CLS.
Conclusion: SILS could be a more safe and reliable surgical technique than CLS for sigmoid colon and rectal cancer. However, further high-quality studies between these two techniques need to be further developed.
Keywords: Laparoscopic surgery; Meta-analysis; Sigmoid colon and rectal cancer; Single-incision.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures




References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
