

Low-Dose Methotrexate for the Prevention of Atherosclerotic Events
- PMID: 30415610
- PMCID: PMC6587584
- DOI: 10.1056/NEJMoa1809798
Low-Dose Methotrexate for the Prevention of Atherosclerotic Events
Abstract
Background: Inflammation is causally related to atherothrombosis. Treatment with canakinumab, a monoclonal antibody that inhibits inflammation by neutralizing interleukin-1β, resulted in a lower rate of cardiovascular events than placebo in a previous randomized trial. We sought to determine whether an alternative approach to inflammation inhibition with low-dose methotrexate might provide similar benefit.
Methods: We conducted a randomized, double-blind trial of low-dose methotrexate (at a target dose of 15 to 20 mg weekly) or matching placebo in 4786 patients with previous myocardial infarction or multivessel coronary disease who additionally had either type 2 diabetes or the metabolic syndrome. All participants received 1 mg of folate daily. The primary end point at the onset of the trial was a composite of nonfatal myocardial infarction, nonfatal stroke, or cardiovascular death. Near the conclusion of the trial, but before unblinding, hospitalization for unstable angina that led to urgent revascularization was added to the primary end point.
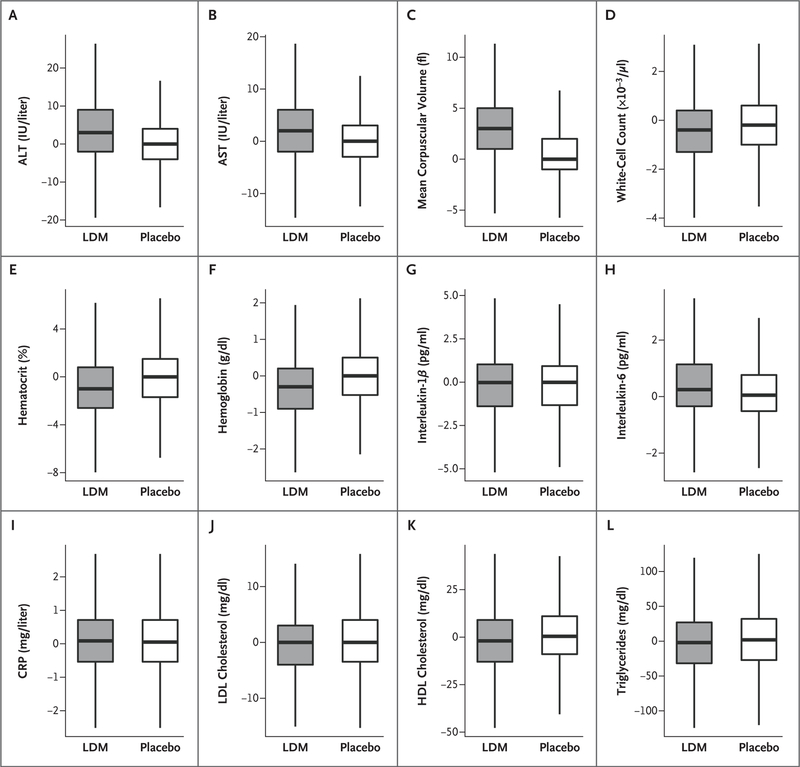
Results: The trial was stopped after a median follow-up of 2.3 years. Methotrexate did not result in lower interleukin-1β, interleukin-6, or C-reactive protein levels than placebo. The final primary end point occurred in 201 patients in the methotrexate group and in 207 in the placebo group (incidence rate, 4.13 vs. 4.31 per 100 person-years; hazard ratio, 0.96; 95% confidence interval [CI], 0.79 to 1.16). The original primary end point occurred in 170 patients in the methotrexate group and in 167 in the placebo group (incidence rate, 3.46 vs. 3.43 per 100 person-years; hazard ratio, 1.01; 95% CI, 0.82 to 1.25). Methotrexate was associated with elevations in liver-enzyme levels, reductions in leukocyte counts and hematocrit levels, and a higher incidence of non-basal-cell skin cancers than placebo.
Conclusions: Among patients with stable atherosclerosis, low-dose methotrexate did not reduce levels of interleukin-1β, interleukin-6, or C-reactive protein and did not result in fewer cardiovascular events than placebo. (Funded by the National Heart, Lung, and Blood Institute; CIRT ClinicalTrials.gov number, NCT01594333.).
Copyright © 2018 Massachusetts Medical Society.
Figures

Comment in
-
No benefit of methotrexate on the risk of cardiovascular events.Nat Rev Cardiol. 2019 Jan;16(1):2-3. doi: 10.1038/s41569-018-0133-6. Nat Rev Cardiol. 2019. PMID: 30487542 No abstract available.
-
Methotrexate for Prevention of Cardiovascular Events.N Engl J Med. 2019 Jun 6;380(23):2276-2277. doi: 10.1056/NEJMc1905061. N Engl J Med. 2019. PMID: 31167066 No abstract available.
-
Methotrexate for Prevention of Cardiovascular Events.N Engl J Med. 2019 Jun 6;380(23):2277. doi: 10.1056/NEJMc1905061. N Engl J Med. 2019. PMID: 31167067 No abstract available.
-
Methotrexate: what are the true risks of treatment?Ann Rheum Dis. 2020 Oct;79(10):1267-1268. doi: 10.1136/annrheumdis-2020-217207. Epub 2020 Jul 1. Ann Rheum Dis. 2020. PMID: 32611600 No abstract available.
References
-
- Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med 2005;352:1685–95. - PubMed
-
- Ridker PM, Everett BM, Thuren T, et al. Antiinflammatory therapy with canakinumab for atherosclerotic disease. N Engl J Med 2017;377:1119–31. - PubMed
-
- Ridker PM, MacFadyen JG, Everett BM, Libby P, Thuren T, Glynn RJ. Relationship of C-reactive protein reduction to cardiovascular event reduction following treatment with canakinumab: a secondary analysis from the CANTOS randomized controlled trial. Lancet 2018;391:319–28. - PubMed
-
- Ridker PM, Libby P, MacFadyen JG, et al. Modulation of the interleukin-6 signalling pathway and incidence rates of atherosclerotic events and all-cause mortality: analyses from the Canakinumab Anti-inflammatory Thrombosis Outcomes Study (CANTOS). Eur Heart J 2018;39: 3499–507. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials