

Temporal patterns in the risk of chronic health conditions in survivors of childhood cancer diagnosed 1970-99: a report from the Childhood Cancer Survivor Study cohort
- PMID: 30416076
- PMCID: PMC6309183
- DOI: 10.1016/S1470-2045(18)30537-0
Temporal patterns in the risk of chronic health conditions in survivors of childhood cancer diagnosed 1970-99: a report from the Childhood Cancer Survivor Study cohort
Erratum in
-
Correction to Lancet Oncol 2018; 19: 1590-601.Lancet Oncol. 2019 Jan;20(1):e10. doi: 10.1016/S1470-2045(18)30928-8. Lancet Oncol. 2019. PMID: 30614470 No abstract available.
Abstract
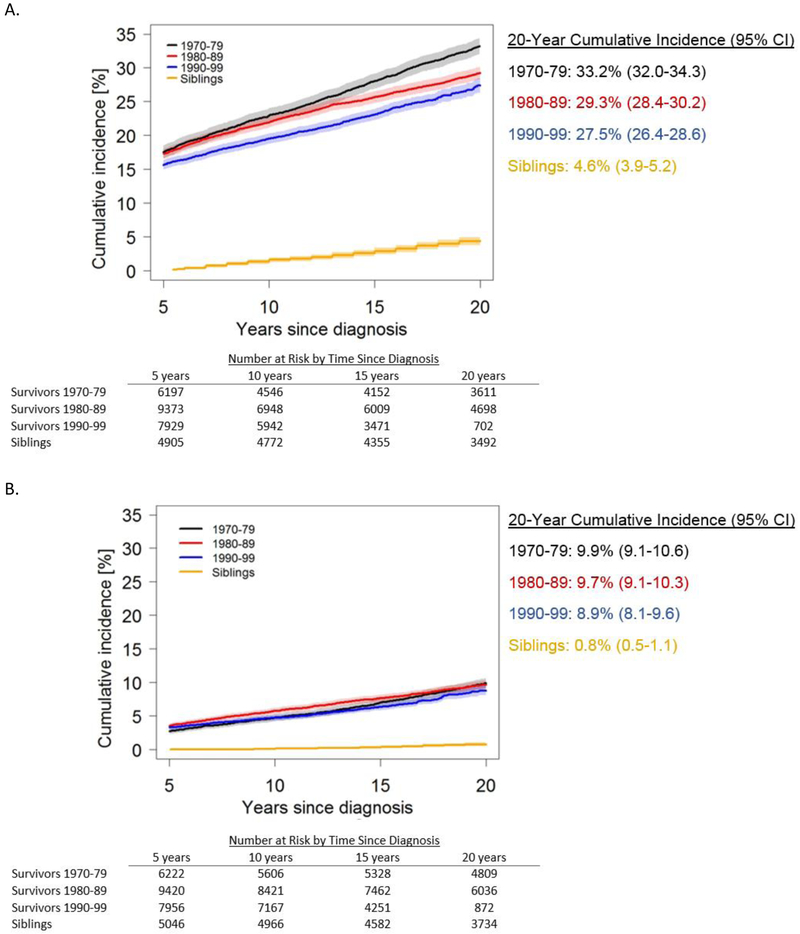
Background: Treatments for childhood cancer have evolved over the past 50 years, with the goal of maximising the proportion of patients who achieve long-term survival, while minimising the adverse effects of therapy. We aimed to assess incidence patterns of serious chronic health conditions in long-term survivors of childhood cancer across three decades of diagnosis and treatment.
Methods: We used data from the Childhood Cancer Survivor Study, a retrospective cohort with longitudinal follow-up of 5-year survivors of common childhood cancers (leukaemia, tumours of the CNS, Hodgkin lymphoma, non-Hodgkin lymphoma, Wilms tumour, neuroblastoma, soft tissue sarcoma, or bone tumours) who were diagnosed before the age of 21 years and from 1970 to 1999 in North America. We examined the cumulative incidence of severe to fatal chronic health conditions occurring up to 20 years post-diagnosis among survivors, compared by diagnosis decade. We used multivariable regression models to estimate hazard ratios per diagnosis decade, and we added treatment variables to assess whether treatment changes attenuated associations between diagnosis decade and chronic disease risk.
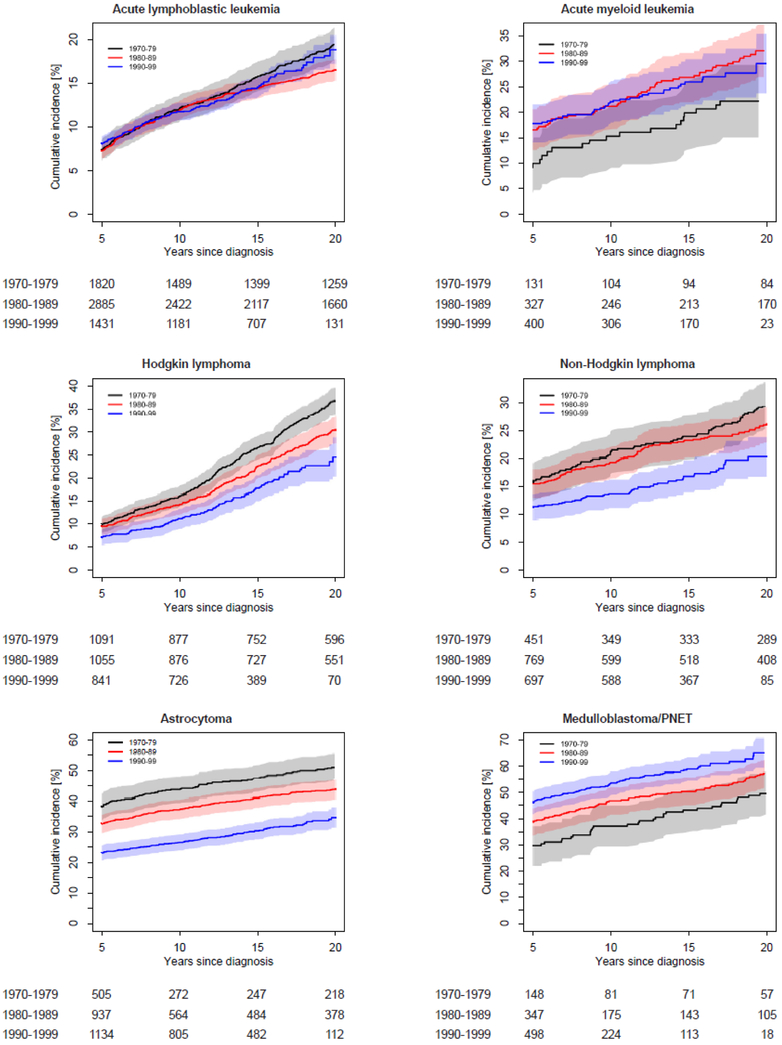
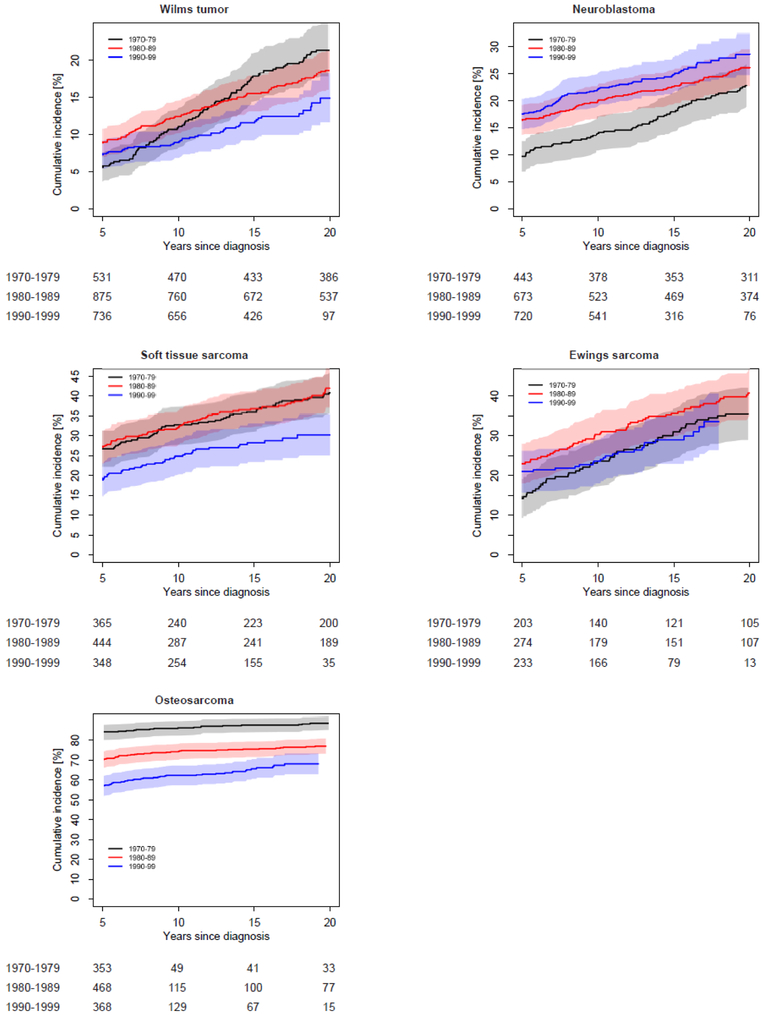
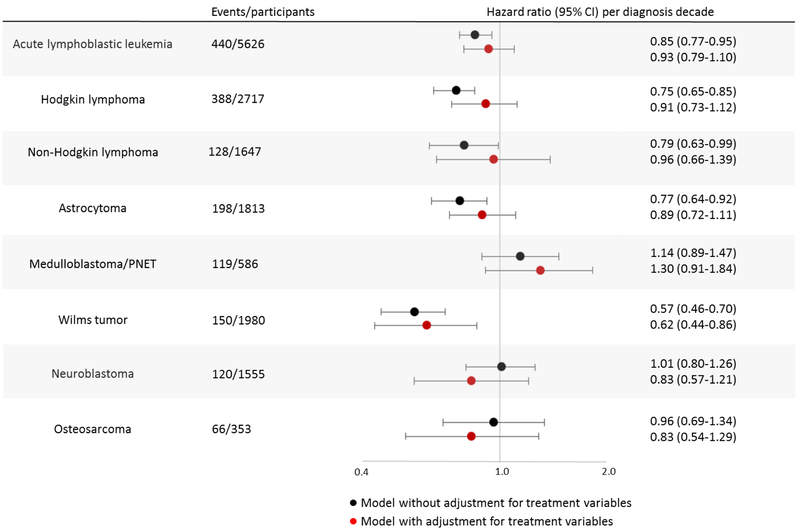
Findings: Among 23 601 survivors with a median follow-up of 21 years (IQR 15-25), the 20-year cumulative incidence of at least one grade 3-5 chronic condition decreased significantly from 33·2% (95% CI 32·0-34·3) in those diagnosed 1970-79 to 29·3% (28·4-30·2; p<0·0001) in 1980-89, and 27·5% (26·4-28·6; p=0·012 vs 1980-89) in 1990-99. By comparison, the 20-year cumulative incidence of at least one grade 3-5 condition in 5051 siblings was 4·6% (95% CI 3·9-5·2). The 15-year cumulative incidence of at least one grade 3-5 condition was lower for survivors diagnosed 1990-99 compared with those diagnosed 1970-79 for Hodgkin lymphoma (17·7% [95% CI 15·0-20·5] vs 26·4% [23·8-29·1]; p<0·0001), non-Hodgkin lymphoma (16·9% [14·0-19·7] vs 23·8% [19·9-27·7]; p=0.0053), astrocytoma (30·5% [27·8-33·2] vs 47·3% [42·9-51·7]; p<0·0001), Wilms tumour (11·9% [9·5-14·3] vs 17·6% [14·3-20·8]; p=0·034), soft tissue sarcoma (28·3% [23·5-33·1] vs 36·5% [31·5-41·4]; p=0·021), and osteosarcoma (65·6% [60·6-70·6] vs 87·5% [84·1-91·0]; p<0·0001). By contrast, the 15-year cumulative incidence of at least one grade 3-5 condition was higher (1990-99 vs 1970-79) for medulloblastoma or primitive neuroectodermal tumour (58·9% [54·4-63·3] vs 42·9% [34·9-50·9]; p=0·00060), and neuroblastoma (25·0% [21·8-28·2] vs 18·0% [14·5-21·6]; p=0·0045). Results were consistent with changes in treatment as a significant mediator of the association between diagnosis decade and risk of grade 3-5 chronic conditions for astrocytoma (HR per decade without treatment in the model = 0·77, 95% CI 0·64-0·92; HR with treatment in the model=0·89, 95% CI 0·72-1·11; pmediation=0·0085) and Hodgkin lymphoma (HR without treatment=0·75, 95% CI 0·65-0·85; HR with treatment=0·91, 95% CI 0·73-1·12; pmediation=0·024). Temporal decreases in 15-year cumulative incidence comparing survivors diagnosed 1970-79 to survivors diagnosed 1990-99 were noted for endocrinopathies (5·9% [5·3-6·4] vs 2·8% [2·5-3·2]; p<0·0001), subsequent malignant neoplasms (2·7% [2·3-3·1] vs 1·9% [1·6-2·2]; p=0·0033), musculoskeletal conditions (5·8% [5·2-6·4] vs 3·3% [2·9-3·6]; p<0·0001), and gastrointestinal conditions (2·3% [2·0-2·7] vs 1·5% [1·3-1·8]; p=0·00037), while hearing loss increased (3·0% [2·6-3·5] vs 5·7% [5·2-6·1]; p<0·0001).
Interpretation: Our results suggest that more recently treated survivors of childhood cancer had improvements in health outcomes, consistent with efforts over the same time period to modify childhood cancer treatment regimens to maximise overall survival, while reducing risk of long-term adverse events. Continuing advances in cancer therapy offer promise of further reducing the risk of long-term adverse events in childhood cancer survivors. However, achieving long-term survival for childhood cancer continues to come at a cost for many survivors, emphasising the importance of long-term follow-up care for this population.
Funding: National Cancer Institute and the American Lebanese-Syrian Associated Charities.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Long-term follow-up care needed for children surviving cancer: still a long way to go.Lancet Oncol. 2018 Dec;19(12):1546-1548. doi: 10.1016/S1470-2045(18)30657-0. Epub 2018 Nov 8. Lancet Oncol. 2018. PMID: 30416075 No abstract available.
References
-
- SEER Cancer Statistics Review (CSR), 1975-2014 Bethesda, MD: National Cancer Institute (http://seer.cancer.gov/csr/1975_2014/).
-
- Geenen MM, Cardous-Ubbink MC, Kremer LCM, et al. Medical assessment of adverse health outcomes in long-term survivors of childhood cancer. JAMA 2007; 297: 2705–15. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
