

Genomically annotated risk model for advanced renal-cell carcinoma: a retrospective cohort study
- PMID: 30416077
- PMCID: PMC6701184
- DOI: 10.1016/S1470-2045(18)30648-X
Genomically annotated risk model for advanced renal-cell carcinoma: a retrospective cohort study
Abstract
Background: The Memorial Sloan Kettering Cancer Center (MSKCC) risk model is an established prognostic tool for metastatic renal-cell carcinoma that integrates clinical and laboratory data, but is agnostic to tumour genomics. Several mutations, including BAP1 and PBRM1, have prognostic value in renal-cell carcinoma. Using two independent clinical trial datasets of patients with metastatic renal-cell carcinoma, we aimed to study whether the addition of the mutation status for several candidate prognostic genes to the MSKCC model could improve the model's prognostic performance.
Methods: In this retrospective cohort study, we used available formalin-fixed paraffin-embedded tumour tissue and clinical outcome data from patients with metastatic renal-cell carcinoma assigned to treatment with tyrosine kinase inhibitors in the COMPARZ trial (training cohort; n=357) and RECORD-3 trial (validation cohort; n=258). Eligible patients in both trials were treatment-naive; had histologically confirmed, advanced, or metastatic renal-cell carcinoma; and a Karnofsky performance status score of at least 70. For each cohort, data from patients in all treatment groups (sunitinib and pazopanib in the training cohort, and everolimus and sunitinib in the validation cohort) were pooled for this analysis. In the training cohort, tumour tissue was used to evaluate somatic mutations by next-generation sequencing, and the association between cancer-specific outcomes (overall survival, progression-free survival, and overall response) and the mutation status of six genes of interest (BAP1, PBRM1, TP53, TERT, KDM5C, and SETD2) was tested. Only those genes with prognostic value in this setting were added to the MSKCC risk model to create a genomically annotated version. The validation cohort was used to independently test the prognostic value of the annotated model compared with the original MSKCC risk model.
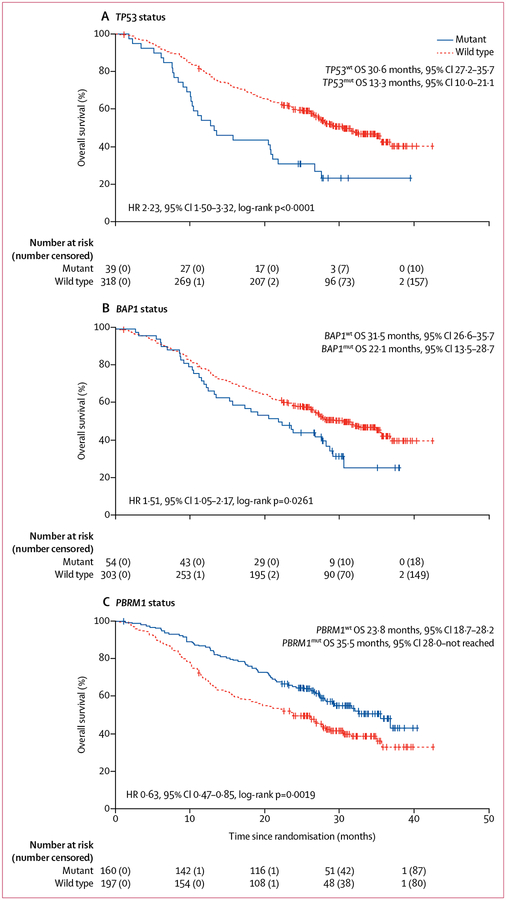
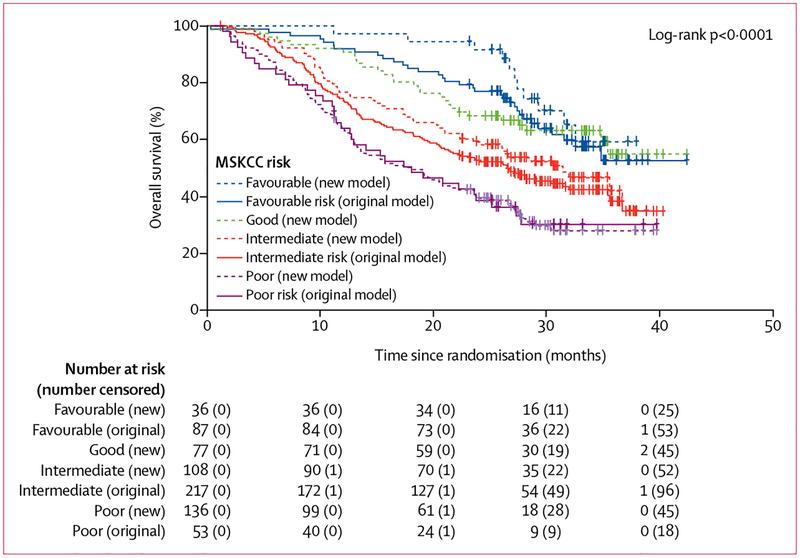
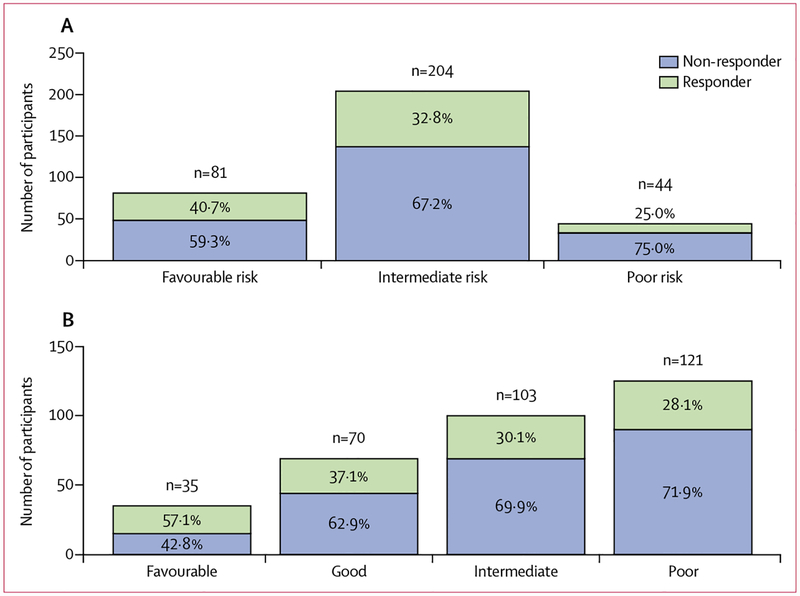
Findings: 357 (32%) of 1110 patients assigned to protocol treatment in the COMPARZ study between August, 2008, and September, 2011, were evaluable for mutation status and clinical outcomes in the training cohort. The independent validation cohort included 258 (55%) of 471 evaluable patients, enrolled between October, 2009, and June, 2011, on the RECORD-3 study. In the training cohort, the presence of any mutation in BAP1 or TP53, or both, and absence of any mutation in PBRM1 were prognostic in terms of overall survival (TP53wt/BAP1mut, TP53mut/BAP1wt o TP53mut/BAP1mut vs TP53wt/BAP1wt hazard ratio [HR] 1·57, 95% CI 1·21-2·04; p=0·0008; PBRM1wt vs PBRMmut, HR 1·58, 1·16-2·14; p=0·0035). The mutation status for these three prognostic genes were added to the original MSKCC risk model to create a genomically annotated version. Distribution of participants in the training cohort into the three risk groups of the original MSKCC model changed from 87 (24%) of 357 patients deemed at favourable risk, 217 (61%) at intermediate risk, and 53 (15%) at poor risk, to distribution across four risk groups in the genomically annotated risk model, with 36 (10%) of 357 deemed at favourable risk, 77 (22%) at good risk, 108 (30%) at intermediate risk, and 136 (38%) at poor risk. Addition of genomic information improved model performance for predicting overall survival (C-index: original model, 0·595 [95% CI 0·557-0·634] vs new model, 0·637 [0·595-0·679]) and progression-free survival (0·567 [95% CI 0·529-0·604] vs 0·602 [0·560-0·643]) with adequate discrimination of the proportion of patients who achieved an objective response (Cochran-Armitage one-sided p=0·0014). Analyses in the validation cohort confirmed the superiority of the genomically annotated risk model over the original version.
Interpretation: The mutation status of BAP1, PBRM1, and TP53 has independent prognostic value in patients with advanced or metastatic renal-cell carcinoma treated with first-line tyrosine kinase inhibitors. Improved stratification of patients across risk groups by use of a genomically annotated model including the mutational status of these three genes warrants further investigation in prospective trials and could be of use as a model to stratify patients with metastatic renal-cell carcinoma in clinical trials.
Funding: Novartis Pharmaceuticals Corporation, MSKCC Support Grant/Core Grant, and the J Randall & Kathleen L MacDonald Research Fund.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Biomarkers in renal-cell carcinoma: building on clinical paradigms.Lancet Oncol. 2018 Dec;19(12):1560-1561. doi: 10.1016/S1470-2045(18)30674-0. Epub 2018 Nov 8. Lancet Oncol. 2018. PMID: 30416074 No abstract available.
References
-
- Sato Y, Yoshizato T, Shiraishi Y, et al. Integrated molecular analysis of clear-cell renal cell carcinoma. Nat Genet 2013; 45: 860–67. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
