

Surgical treatment of bronchial rupture in blunt chest trauma: a review of literature
- PMID: 30416808
- PMCID: PMC6196165
- DOI: 10.21037/jtd.2018.08.22
Surgical treatment of bronchial rupture in blunt chest trauma: a review of literature
Abstract
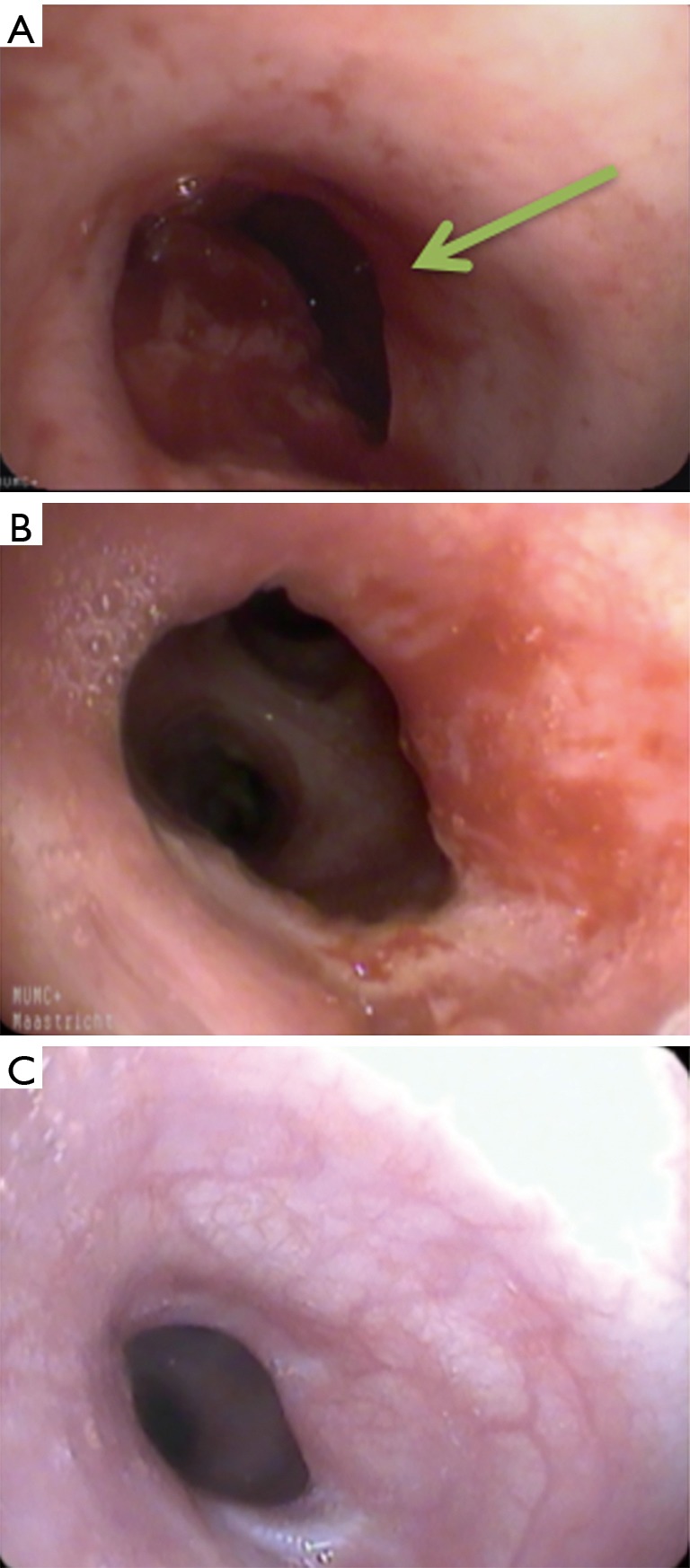
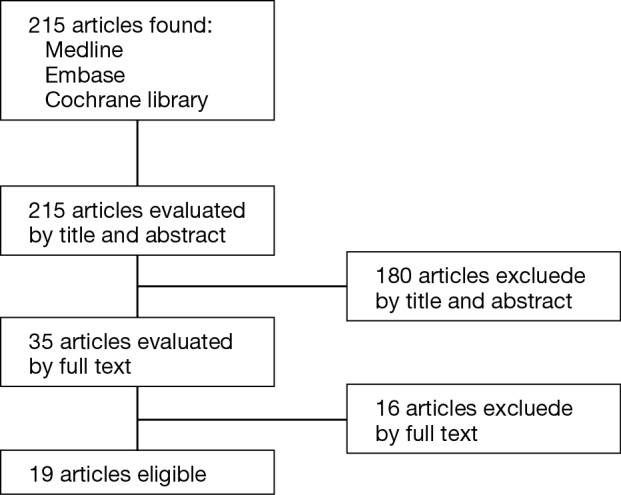
Bronchial rupture by blunt chest trauma is rare. We present a case of bronchial injury after blunt chest trauma that was repaired surgically by primary reconstruction. We performed a review of literature to verify if primary reconstruction is suitable for the treatment of adult patients with blunt bronchial injury. A systematic search was conducted to identify cohort studies of bronchial rupture after blunt chest trauma in adult patients between 1985 and 2016 (n=215 articles). Studies were included concerning four or more patients and in case patient data could be extracted. This resulted in 19 articles for final review, consisting of 155 patients. Mean age of 155 patients was 28 (range, 18-60) years. The main bronchus was mostly injured (81%), in 5% including an injury of the trachea and in 14% lobar bronchi injury. Surgical repair was performed in 95% of patients: primary anastomosis in 72%, pneumonectomy in 15%, lobectomy or sleeve resection in 12% and other in 1%. Perioperative mortality rate was 10%. Other complications occurred in 17% (empyema, rebleeding, stenosis and fistula, among others). Data concerning the occurrence of long-term complications or long-term follow-up was not found. Statistical evaluation could not be performed due to lack of consistent patient data. No strong recommendations regarding type and timing of surgery can be made based on the available literature. Based on our multidisciplinary opinion we would advocate primary anastomosis in case of stable vital signs with the goal to preserve healthy lung parenchyma. Moreover, it may be considered transferring these rare cases to an experienced thoracic and trauma surgery center.
Keywords: Bronchus; review; rupture; surgery; trauma.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures


References
-
- van Roozendaal LM, van Gool MH, Sprooten RT, et al. The completely transected left main bronchus is visualized after mediastinal dissection of pulmonary veins, aortic arch and main pulmonary artery. Asvide 2018;5:783. Available online: http://www.asvide.com/article/view/27401
Publication types
LinkOut - more resources
Full Text Sources