

Association of MRI T2 Signal Intensity With Desmoid Tumor Progression During Active Observation: A Retrospective Cohort Study
- PMID: 30418203
- PMCID: PMC6736761
- DOI: 10.1097/SLA.0000000000003073
Association of MRI T2 Signal Intensity With Desmoid Tumor Progression During Active Observation: A Retrospective Cohort Study
Abstract
Objective: The aim of this study was to identify predictors of desmoid progression during observation.
Summary of background data: Untreated desmoids can grow, remain stable, or regress, but reliable predictors of behavior have not been identified.
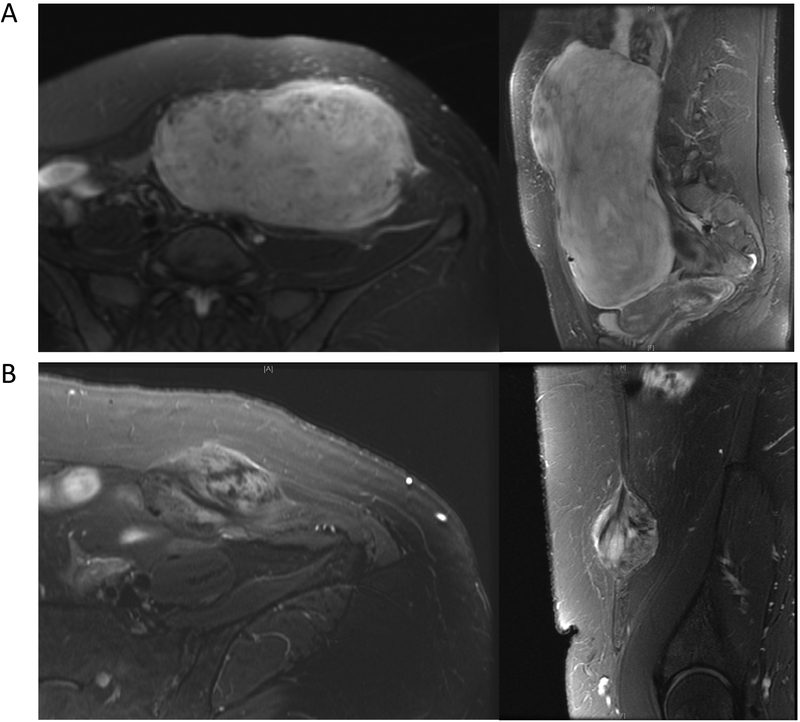
Methods: Primary or recurrent desmoid patients were identified retrospectively from an institutional database. In those managed with active observation who underwent serial magnetic resonance imaging (MRIs) with T2-weighted sequences, baseline tumor size was recorded, and 2 radiologists independently estimated the percentage of tumor volume showing hyperintense T2 signal at baseline. Associations of clinical or radiographic characteristics with progression-free survival (PFS; by RECIST) were evaluated by Cox regression and Kaplan-Meier statistics.
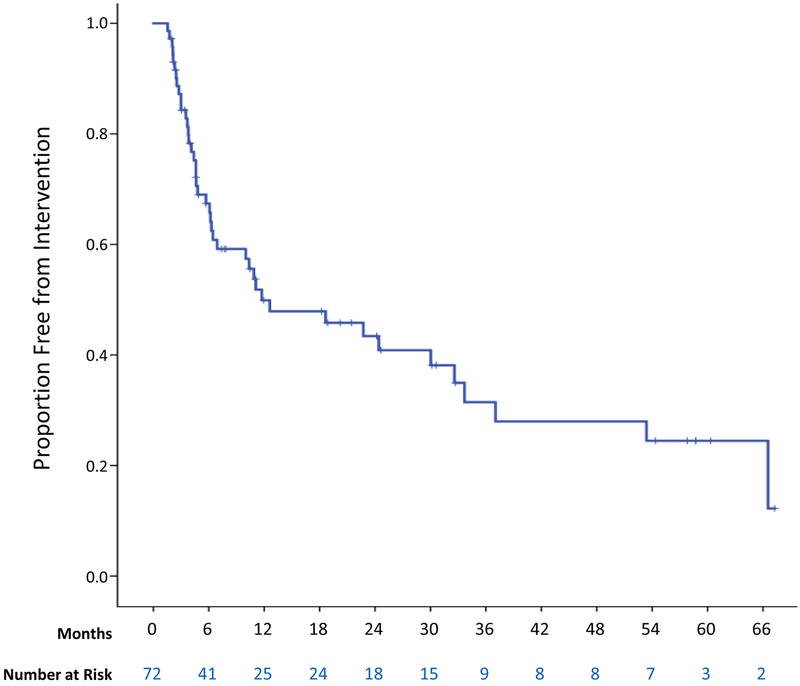
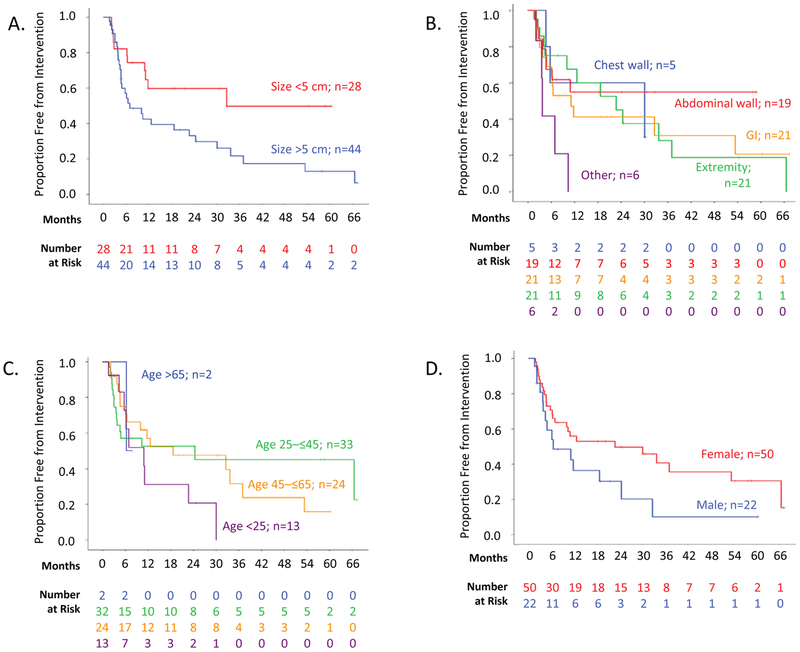
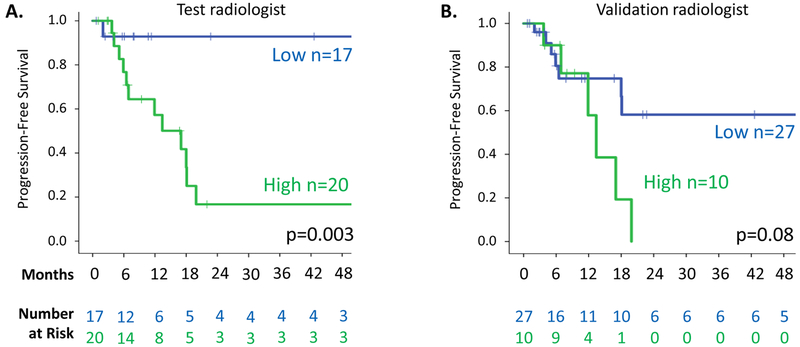
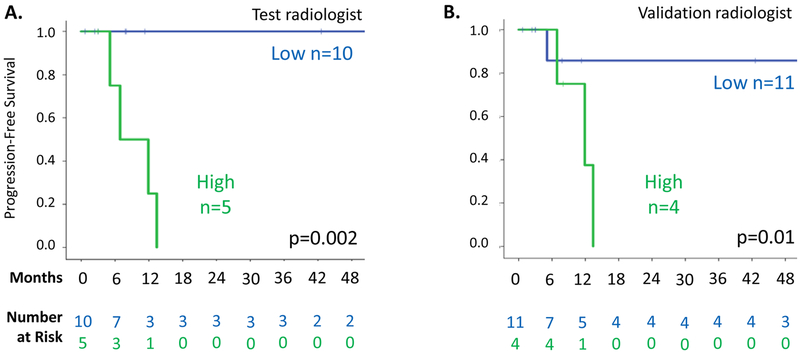
Results: Among 160 patients with desmoids, 72 were managed with observation, and 37 of these had serial MRI available for review. Among these 37 patients, median age was 35 years and median tumor size was 4.7 cm; all tumors were extra-abdominal (41% in abdominal wall). Although PFS was not associated with size, site, or age, it was strongly associated with hyperintense T2 signal in ≥90% versus <90% of baseline tumor volume (as defined by the "test" radiologist; hazard ratio = 11.3, P = 0.003). For patients in the ≥90% group (n = 20), 1-year PFS was 55%, compared with 94% in the <90% group (n = 17). The percentage of baseline tumor volume with hyperintense T2 signal defined by a validation radiologist correlated with results of the test radiologist (ρ = 0.75).
Conclusion: The percent tumor volume characterized by hyperintense T2 signal is associated with desmoid progression during observation and may help distinguish patients who would benefit from early intervention from those who may be reliably observed.
Conflict of interest statement
Figures
References
-
- Wu C, Amini-Nik S, Nadesan P, et al. Aggressive fibromatosis (desmoid tumor) is derived from mesenchymal progenitor cells. Cancer Res 2010; 70(19):7690–8. - PubMed
-
- Li M, Cordon-Cardo C, Gerald WL, et al. Desmoid fibromatosis is a clonal process. Hum Pathol 1996; 27(9):939–43. - PubMed
-
- Merchant NB, Lewis JJ, Woodruff JM, et al. Extremity and trunk desmoid tumors: a multifactorial analysis of outcome. Cancer 1999; 86(10):2045–52. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
