

Development and Validation of a Deep Learning-based Automatic Detection Algorithm for Active Pulmonary Tuberculosis on Chest Radiographs
- PMID: 30418527
- PMCID: PMC6695514
- DOI: 10.1093/cid/ciy967
Development and Validation of a Deep Learning-based Automatic Detection Algorithm for Active Pulmonary Tuberculosis on Chest Radiographs
Abstract
Background: Detection of active pulmonary tuberculosis on chest radiographs (CRs) is critical for the diagnosis and screening of tuberculosis. An automated system may help streamline the tuberculosis screening process and improve diagnostic performance.
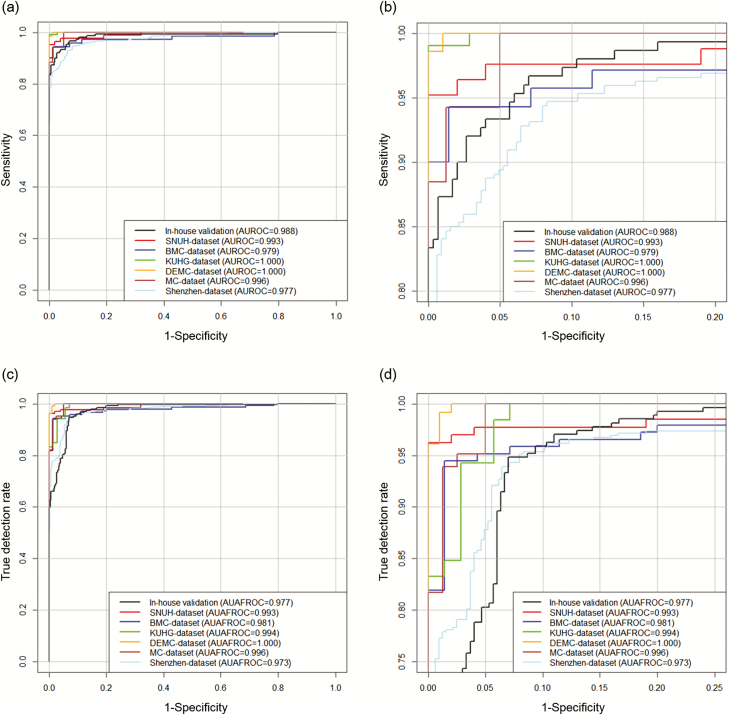
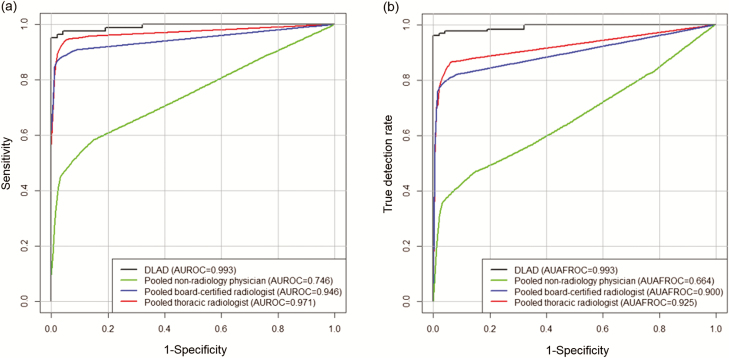
Methods: We developed a deep learning-based automatic detection (DLAD) algorithm using 54c221 normal CRs and 6768 CRs with active pulmonary tuberculosis that were labeled and annotated by 13 board-certified radiologists. The performance of DLAD was validated using 6 external multicenter, multinational datasets. To compare the performances of DLAD with physicians, an observer performance test was conducted by 15 physicians including nonradiology physicians, board-certified radiologists, and thoracic radiologists. Image-wise classification and lesion-wise localization performances were measured using area under the receiver operating characteristic (ROC) curves and area under the alternative free-response ROC curves, respectively. Sensitivities and specificities of DLAD were calculated using 2 cutoffs (high sensitivity [98%] and high specificity [98%]) obtained through in-house validation.
Results: DLAD demonstrated classification performance of 0.977-1.000 and localization performance of 0.973-1.000. Sensitivities and specificities for classification were 94.3%-100% and 91.1%-100% using the high-sensitivity cutoff and 84.1%-99.0% and 99.1%-100% using the high-specificity cutoff. DLAD showed significantly higher performance in both classification (0.993 vs 0.746-0.971) and localization (0.993 vs 0.664-0.925) compared to all groups of physicians.
Conclusions: Our DLAD demonstrated excellent and consistent performance in the detection of active pulmonary tuberculosis on CR, outperforming physicians, including thoracic radiologists.
Keywords: chest radiograph; computer-aided detection; deep learning; tuberculosis.
© The Author(s) 2018. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
Comment in
-
Development and Validation of a Deep Learning System for Detection of Active Pulmonary Tuberculosis on Chest Radiographs: Clinical and Technical Considerations.Clin Infect Dis. 2019 Aug 16;69(5):748-750. doi: 10.1093/cid/ciy969. Clin Infect Dis. 2019. PMID: 30418534 No abstract available.
References
-
- World Health Organization. Global tuberculosis report 2017. Geneva, Switzerland: WHO; 2017.
-
- World Health Organization. Systematic screening for active tuberculosis: principles and recommendations. Geneva, Switzerland: WHO; 2013. - PubMed
-
- den Boon S, White NW, van Lill SW, et al. . An evaluation of symptom and chest radiographic screening in tuberculosis prevalence surveys. Int J Tuberc Lung Dis 2006; 10:876–82. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
