

Learning Domain Shift in Simulated and Clinical Data: Localizing the Origin of Ventricular Activation From 12-Lead Electrocardiograms
- PMID: 30418900
- PMCID: PMC6601334
- DOI: 10.1109/TMI.2018.2880092
Learning Domain Shift in Simulated and Clinical Data: Localizing the Origin of Ventricular Activation From 12-Lead Electrocardiograms
Abstract
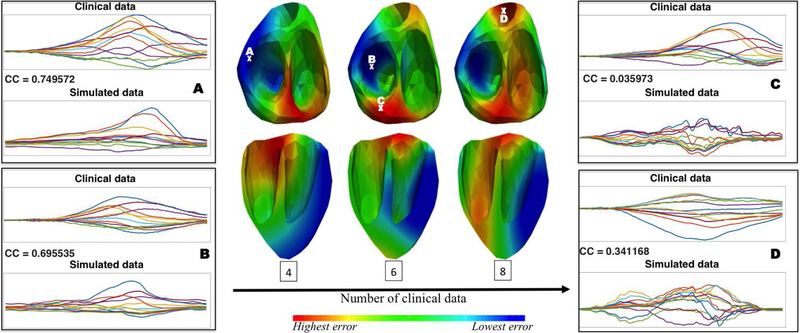
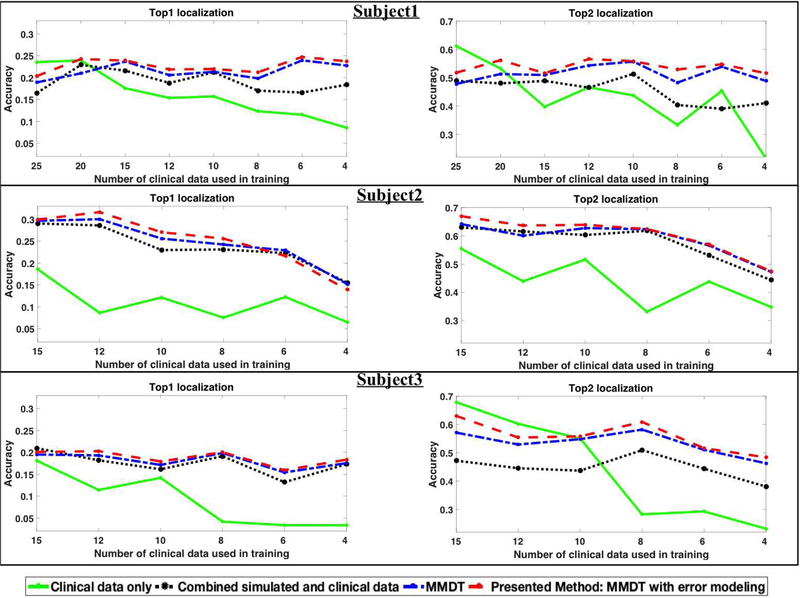
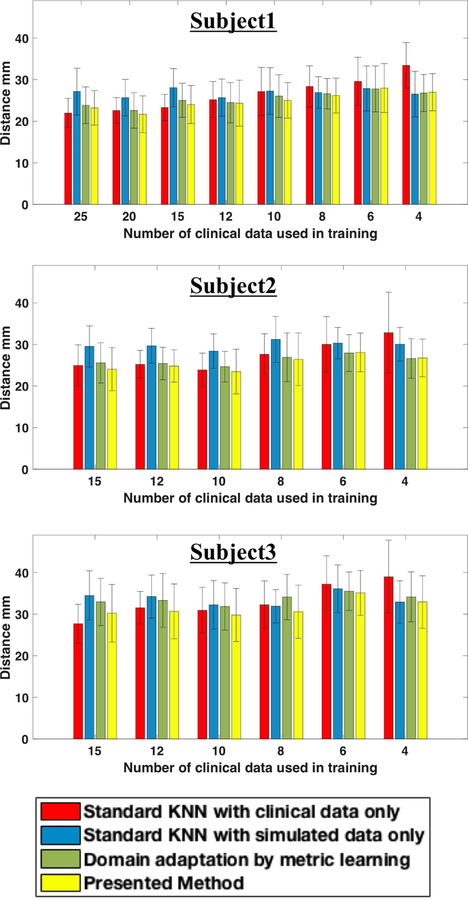
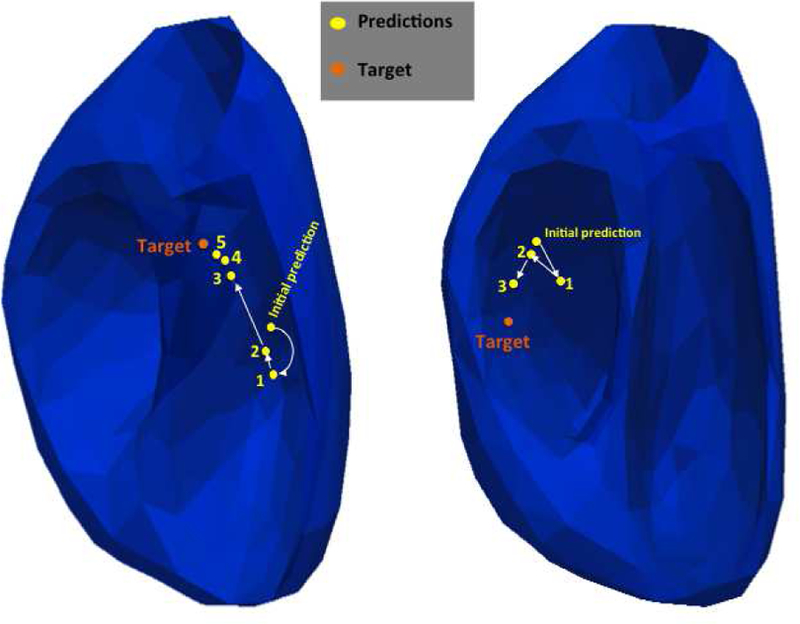
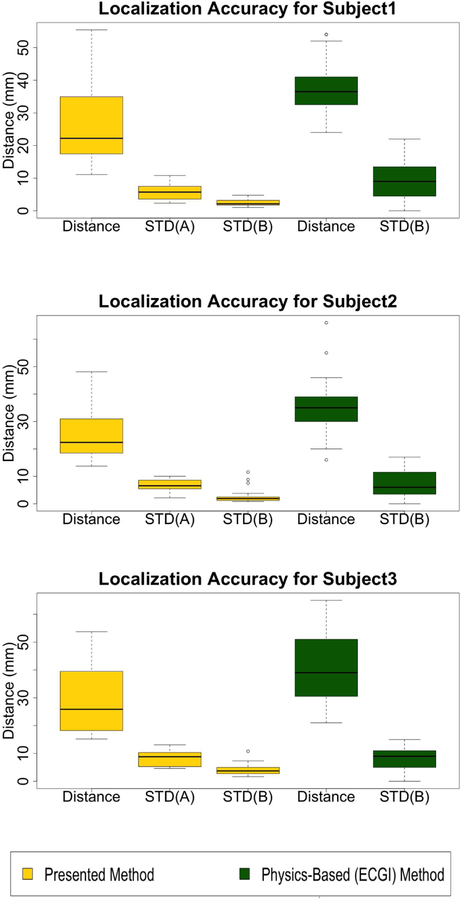
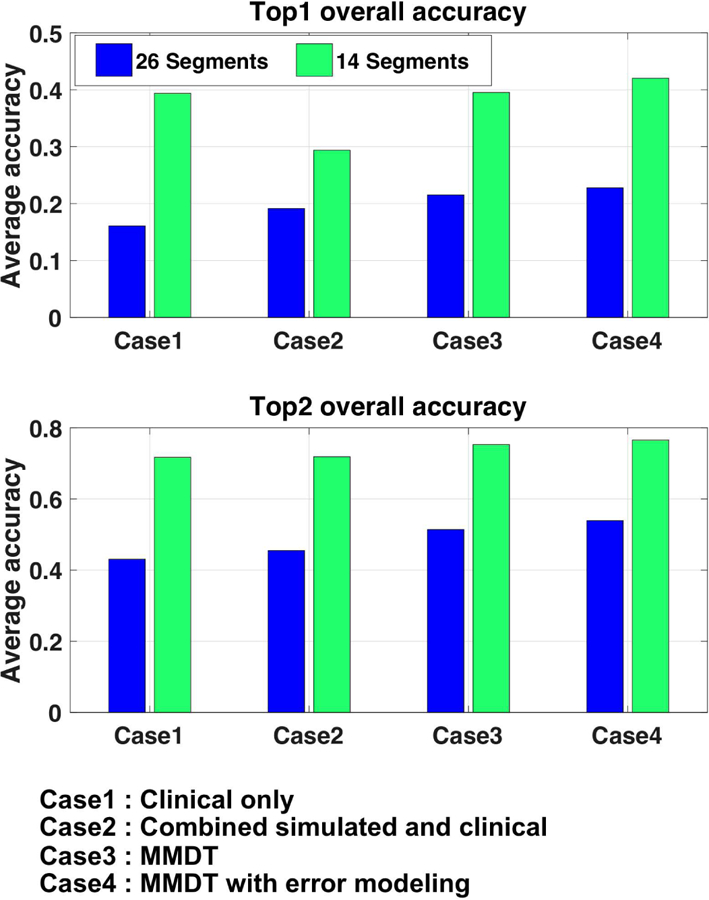
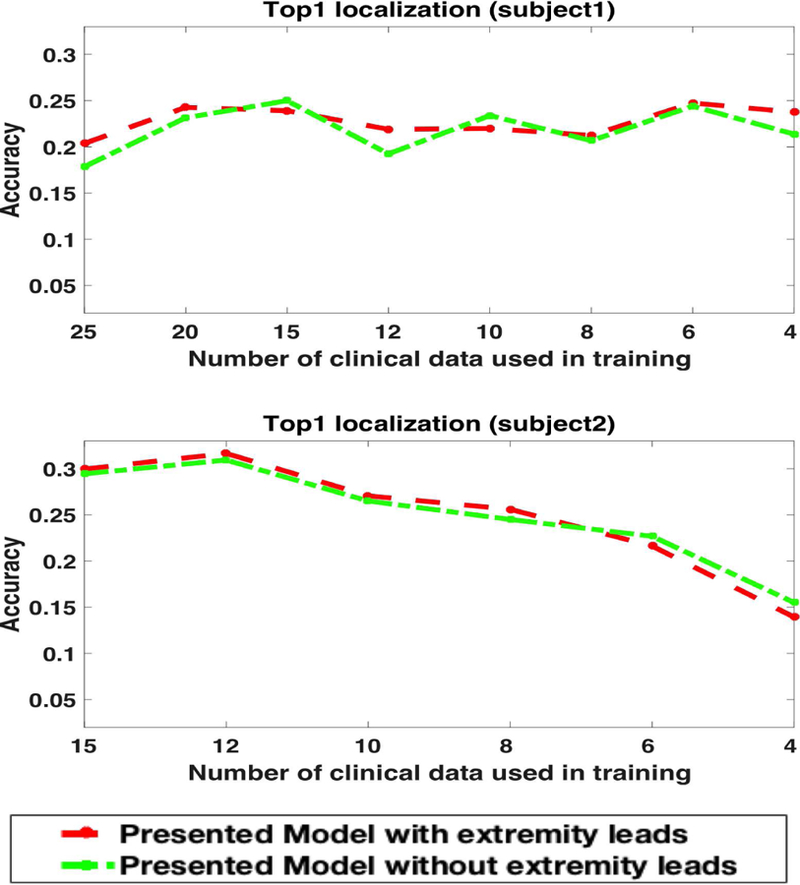
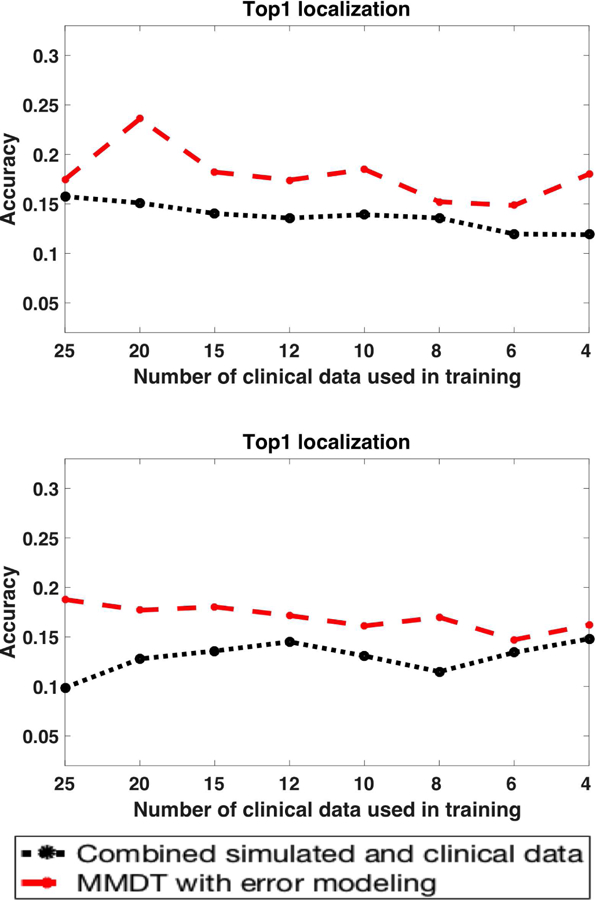
Building a data-driven model to localize the origin of ventricular activation from 12-lead electrocardiograms (ECG) requires addressing the challenge of large anatomical and physiological variations across individuals. The alternative of a patient-specific model is, however, difficult to implement in clinical practice because the training data must be obtained through invasive procedures. In this paper, we present a novel approach that overcomes this problem of the scarcity of clinical data by transferring the knowledge from a large set of patient-specific simulation data while utilizing domain adaptation to address the discrepancy between the simulation and clinical data. The method that we have developed quantifies non-uniformly distributed simulation errors, which are then incorporated into the process of domain adaptation in the context of both classification and regression. This yields a quantitative model that, with the addition of 12-lead ECG data from each patient, provides progressively improved patient-specific localizations of the origin of ventricular activation. We evaluated the performance of the presented method in localizing 75 pacing sites on three in-vivo premature ventricular contraction (PVC) patients. We found that the presented model showed an improvement in localization accuracy relative to a model trained on clinical ECG data alone or a model trained on combined simulation and clinical data without considering domain shift. Furthermore, we demonstrated the ability of the presented model to improve the real-time prediction of the origin of ventricular activation with each added clinical ECG data, progressively guiding the clinician towards the target site.
Figures

Similar articles
-
A "two-step classification" machine learning method for non-invasive localization of premature ventricular contraction origins based on 12-lead ECG.J Interv Card Electrophysiol. 2024 Apr;67(3):457-470. doi: 10.1007/s10840-023-01551-7. Epub 2023 Apr 25. J Interv Card Electrophysiol. 2024. PMID: 37097585
-
Localization of Origins of Premature Ventricular Contraction by Means of Convolutional Neural Network From 12-Lead ECG.IEEE Trans Biomed Eng. 2018 Jul;65(7):1662-1671. doi: 10.1109/TBME.2017.2756869. Epub 2017 Sep 25. IEEE Trans Biomed Eng. 2018. PMID: 28952932 Free PMC article.
-
Localization of origins of premature ventricular contraction in the whole ventricle based on machine learning and automatic beat recognition from 12-lead ECG.Physiol Meas. 2020 Jun 10;41(5):055007. doi: 10.1088/1361-6579/ab86d7. Physiol Meas. 2020. PMID: 32252035
-
Twelve-lead electrocardiographic localization of idiopathic premature ventricular contraction origins.J Cardiovasc Electrophysiol. 2019 Nov;30(11):2603-2617. doi: 10.1111/jce.14152. Epub 2019 Sep 22. J Cardiovasc Electrophysiol. 2019. PMID: 31502322 Review.
-
Machine Learning for Localization of Premature Ventricular Contraction Origins: A Review.Pacing Clin Electrophysiol. 2024 Nov;47(11):1481-1491. doi: 10.1111/pace.15089. Epub 2024 Oct 20. Pacing Clin Electrophysiol. 2024. PMID: 39428720 Review.
Cited by
-
Improving localization accuracy for non-invasive automated early left ventricular origin localization approach.Front Physiol. 2023 Jun 26;14:1183280. doi: 10.3389/fphys.2023.1183280. eCollection 2023. Front Physiol. 2023. PMID: 37435305 Free PMC article.
-
Reconstruction of three-dimensional biventricular activation based on the 12-lead electrocardiogram via patient-specific modelling.Europace. 2021 Apr 6;23(4):640-647. doi: 10.1093/europace/euaa330. Europace. 2021. PMID: 33241411 Free PMC article.
-
Creation and application of virtual patient cohorts of heart models.Philos Trans A Math Phys Eng Sci. 2020 Jun 12;378(2173):20190558. doi: 10.1098/rsta.2019.0558. Epub 2020 May 25. Philos Trans A Math Phys Eng Sci. 2020. PMID: 32448064 Free PMC article.
-
Training machine learning models with synthetic data improves the prediction of ventricular origin in outflow tract ventricular arrhythmias.Front Physiol. 2022 Aug 12;13:909372. doi: 10.3389/fphys.2022.909372. eCollection 2022. Front Physiol. 2022. PMID: 36035489 Free PMC article.
-
Sequential Factorized Autoencoder for Localizing the Origin of Ventricular Activation From 12-Lead Electrocardiograms.IEEE Trans Biomed Eng. 2020 May;67(5):1505-1516. doi: 10.1109/TBME.2019.2939138. Epub 2019 Sep 3. IEEE Trans Biomed Eng. 2020. PMID: 31494539 Free PMC article.
References
-
- Stevenson WG, “Current treatment of ventricular arrhythmias: state of the art,” Heart Rhythm, vol. 10, no. 12, pp. 1919–1926, 2013. - PubMed
-
- Park KM, Kim YH, and Marchlinski FE, “Using the surface electrocardiogram to localize the origin of idiopathic ventricular tachycardia,” Pacing and Clinical Electrophysiology, vol. 35, no. 12, pp. 1516–1527, 2012. - PubMed
-
- Yokokawa M, Liu TY, Yoshida K, Scott C, Hero A, Good E, Morady F, and Bogun F, “Automated analysis of the 12-lead electrocardiogram to identify the exit site of postinfarction ventricular tachycardia,” Heart Rhythm, vol. 9, no. 3, pp. 330–334, 2012. [Online]. Available: 10.1016/j.hrthm.2011.10.014 - DOI - PubMed
-
- Sapp JL, Bar-Tal M, Howes AJ, Toma JE, El-Damaty A, Warren JW, MacInnis PJ, Zhou S, and Horáček BM, “Real-time localization of ventricular tachycardia origin from the 12-lead electrocardiogram,” JACC: Clinical Electrophysiology, vol. 3, no. 7, pp. 687–699, 2017. - PubMed
-
- Potse M, Linnenbank AC, Peeters HAP, SippensGroenewegen A, and Crimbergen CA, “Continuous localization of cardiac activation sites using a database of multichannel ECG recordings,” IEEE transactions on biomedical engineering, vol. 47, no. 5, pp. 682–689, 2000. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
