

Health care utilization and cost after discharge from a mental health hospital; an RCT comparing community residential aftercare and treatment as usual
- PMID: 30419894
- PMCID: PMC6233284
- DOI: 10.1186/s12888-018-1941-2
Health care utilization and cost after discharge from a mental health hospital; an RCT comparing community residential aftercare and treatment as usual
Abstract
Background: Community residential aftercare (step-down) services can ease the transition after a mental health hospital stay for patients with severe mental illness (SMI).
Aims: To investigate use of community and specialised mental health care services and costs in patients with SMI the first 12 months after discharge from a mental health hospital (MHH), comparing community residential aftercare (CRA) and treatment as usual.
Methods: An open parallel group randomised controlled trial with 41 participants. Data on use of specialist services (hospital, ambulant treatment and outpatient treatment) and community services (residential stays, home help, home care nursing, mental health consultation) were collected from specialist and community registers and health records.
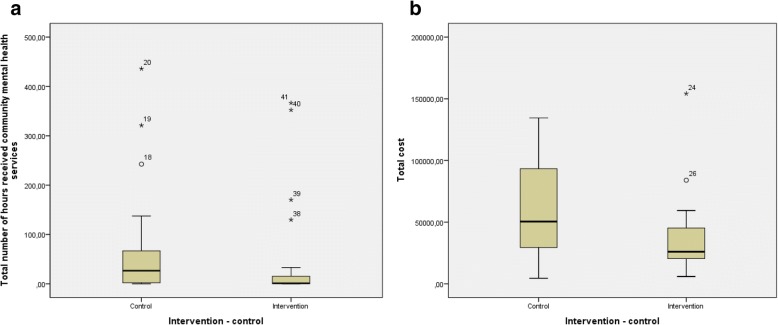
Results: For the primary outcome, utilisation of community mental health services, the intervention group used, on average, 29% fewer hours (mean differences - 21.6 h, 95% CI -93.1 to 44.9, p = .096) with a cost saving of 29% (mean differences - 1845 EUR, 95% CI -8267 to 4171, p = .102), but the estimates were imprecise. For the secondary outcome, the study groups had the same total number of inpatient days (66 days), but the intervention group had on average of 13.4 fewer inpatient days in the mental health hospital (95% CI -29.9 to 0.9. p = .008). The number of inpatient admissions (mean difference - 0.9 admissions, 95% CI -3.5 to 1.5, p = .224) and readmissions (- 0.8, 95% CI -2.5 to 0.9. p = .440) was lower in the intervention group. The intervention group had on average a total cost saving of 38.5% (mean differences - 23,071 EUR, 95% CI -45,450 to 3027. p = .057). A post hoc multivariable regression analysis controlling for baseline characteristics gave a reduction in total cost in favour of the intervention group of - 19,781 EUR (95% CI -44,072 to 4509, p=,107).
Conclusion: In this study, it was not possible to draw a definite conclusion about the effect, due to the small sample and imprecision of the estimates. The direction of the results and size of the point estimate, in addition to findings in other studies, indicates that transferring patients ready for discharge from mental hospital to community residential aftercare can have the potential to reduce total consumption of health services and costs without increased hospital admissions.
Trial registration: Registered in clinicaltrials.gov ( NCT01719354 ).
Keywords: Community residential aftercare; Discharge-ready mental health patients; Severe mental illness; Step-down.
Conflict of interest statement
Ethics approval and consent to participate
This was an open parallel group randomised controlled trial including patients from January 2013 to April 2015. It was approved by the Committee for Medical and Health Research Ethics in Central Norway (2011/1770) and was registered in clinicaltrials.gov (NCT01719354). The patients had to be older than 18 years and they had to sign the informed consent.
Consent for publication
Not applicable.
Competing interests
The first author (ER) worked with the establishment of the CRA as an advisor to the chief officer in the municipality, but has not been involved in the day to day operation of the service. The other authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Cost-effectiveness Analysis of an Aftercare Service vs Treatment-As-Usual for Patients with Severe Mental Disorders.J Ment Health Policy Econ. 2017 Sep 1;20(3):101-110. J Ment Health Policy Econ. 2017. PMID: 28869209 Clinical Trial.
-
Psychiatric inpatient cost of care before and after admission at a residential subacute step-up/step-down mental health facility.J Med Econ. 2019 May;22(5):491-498. doi: 10.1080/13696998.2019.1588126. Epub 2019 Mar 15. J Med Econ. 2019. PMID: 30810050
-
A multicenter randomized controlled trial of aftercare services for severe mental illness: study protocol.BMC Psychiatry. 2013 Jul 1;13:178. doi: 10.1186/1471-244X-13-178. BMC Psychiatry. 2013. PMID: 23816199 Free PMC article. Clinical Trial.
-
Compulsory community treatment to reduce readmission to hospital and increase engagement with community care in people with mental illness: a systematic review and meta-analysis.Lancet Psychiatry. 2018 Dec;5(12):1013-1022. doi: 10.1016/S2215-0366(18)30382-1. Epub 2018 Nov 1. Lancet Psychiatry. 2018. PMID: 30391280 Free PMC article.
-
Severe mental illness and health service utilisation for nonpsychiatric medical disorders: A systematic review and meta-analysis.PLoS Med. 2020 Sep 14;17(9):e1003284. doi: 10.1371/journal.pmed.1003284. eCollection 2020 Sep. PLoS Med. 2020. PMID: 32925912 Free PMC article.
Cited by
-
Health Care Management Models for the Evolution of Hospitalization in Acute Inpatient Psychiatry Units: Comparative Quantitative Study.JMIR Ment Health. 2020 Nov 30;7(11):e15776. doi: 10.2196/15776. JMIR Ment Health. 2020. PMID: 33252351 Free PMC article.
-
Measurement of unnecessary psychiatric readmissions in the context of care transition interventions: a scoping review.BMJ Open. 2021 Feb 8;11(2):e045364. doi: 10.1136/bmjopen-2020-045364. BMJ Open. 2021. PMID: 33558362 Free PMC article.
-
Parent SMART: Effects of residential treatment and an adjunctive parenting intervention on behavioral health services utilization.J Subst Use Addict Treat. 2024 Nov;166:209399. doi: 10.1016/j.josat.2024.209399. Epub 2024 May 16. J Subst Use Addict Treat. 2024. PMID: 38762125 Clinical Trial.
References
-
- Davydow DS, Ribe AR, Pedersen HS, Fenger-Gron M, Cerimele JM, Vedsted P, Vestergaard M. Serious mental illness and risk for hospitalizations and Rehospitalizations for ambulatory care-sensitive conditions in Denmark: a Nationwide population-based cohort study. Med Care. 2016;54(1):90–97. doi: 10.1097/MLR.0000000000000448. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
