

The burden of common variable immunodeficiency disorders: a retrospective analysis of the European Society for Immunodeficiency (ESID) registry data
- PMID: 30419968
- PMCID: PMC6233554
- DOI: 10.1186/s13023-018-0941-0
The burden of common variable immunodeficiency disorders: a retrospective analysis of the European Society for Immunodeficiency (ESID) registry data
Abstract
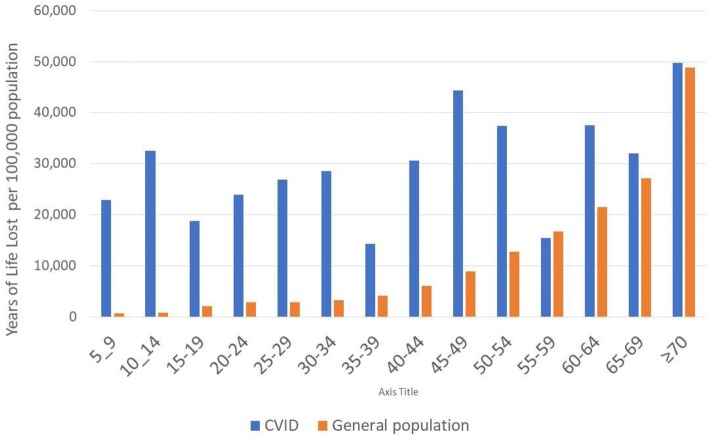
Background: Common variable immunodeficiency disorders (CVID) are a group of rare innate disorders characterized by specific antibody deficiency and increased rates of infections, comorbidities and mortality. The burden of CVID in Europe has not been previously estimated. We performed a retrospective analysis of the European Society for Immunodeficiencies (ESID) registry data on the subset of patients classified by their immunologist as CVID and treated between 2004 and 2014. The registered deaths and comorbidities were used to calculate the annual average age-standardized rates of Years of Life Lost to premature death (YLL), Years Lost to Disability (YLD) and Disability Adjusted Life Years (DALY=YLL + YLD). These outcomes were expressed as a rate per 105 of the CVID cohort (the individual disease burden), and of the general population (the societal disease burden).
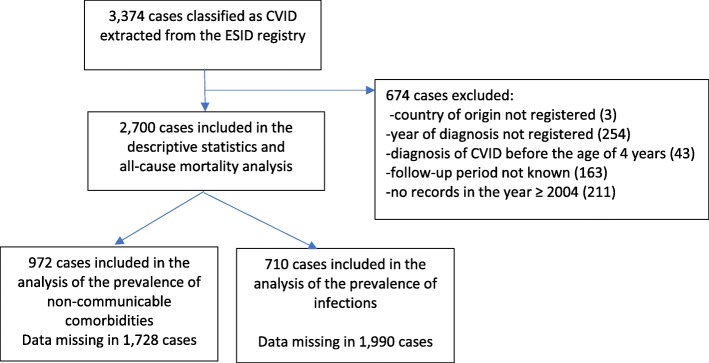
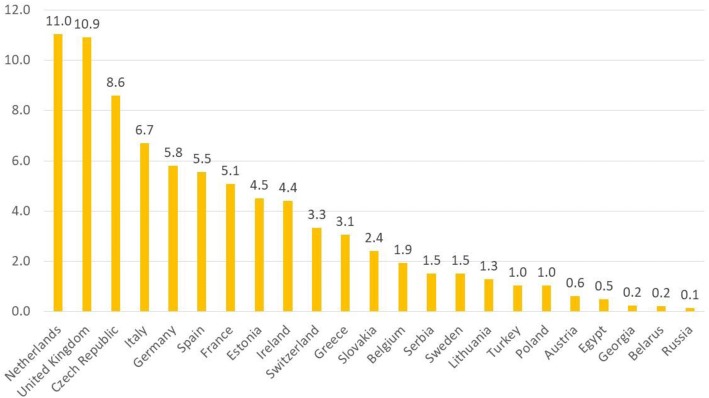
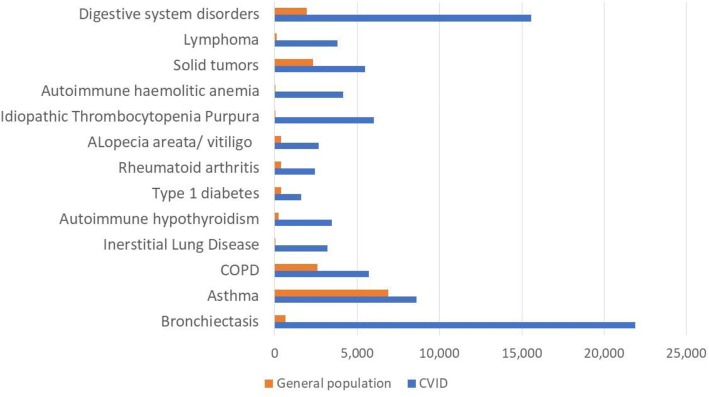
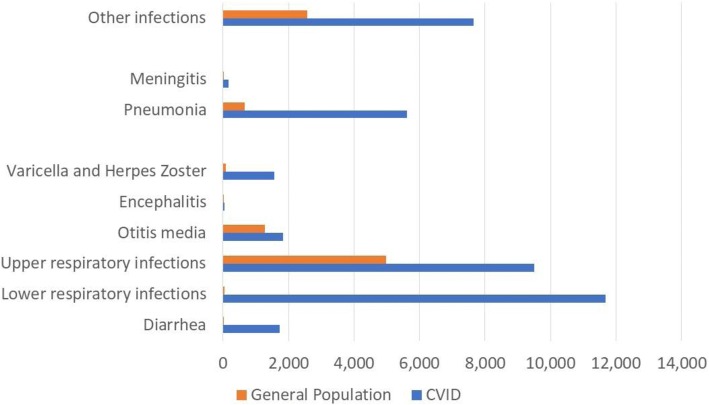
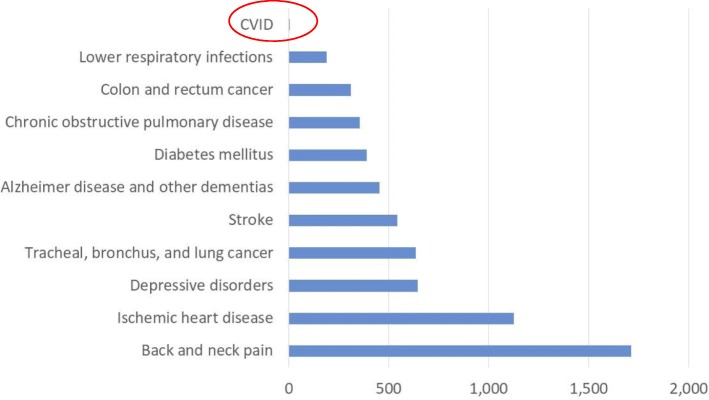
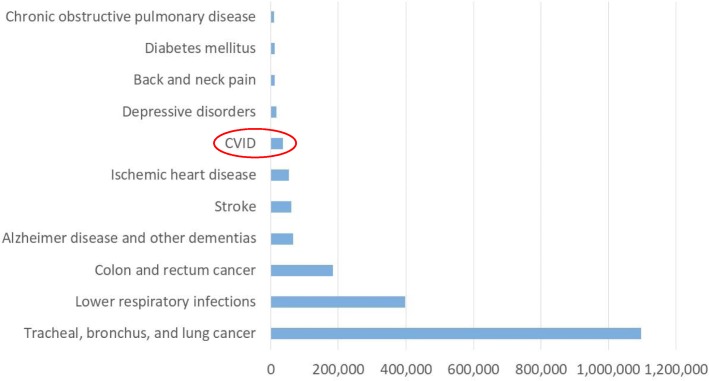
Results: Data of 2700 patients from 23 countries were analysed. Annual comorbidity rates: bronchiectasis, 21.9%; autoimmunity, 23.2%; digestive disorders, 15.6%; solid cancers, 5.5%; lymphoma, 3.8%, exceeded the prevalence in the general population by a factor of 34.0, 7.6, 8.1, 2.4 and 32.6, respectively. The comorbidities of CVID caused 8722 (6069; 12,363) YLD/105 in this cohort, whereas 44% of disability burden was attributable to infections and bronchiectasis. The total individual burden of CVID was 36,785 (33,078, 41,380) DALY/105. With estimated CVID prevalence of ~ 1/ 25,000, the societal burden of CVID ensued 1.5 (1.3, 1.7) DALY/105 of the general population. In exploratory analysis, increased mortality was associated with solid tumor, HR (95% CI): 2.69 (1.10; 6.57) p = 0.030, lymphoma: 5.48 (2.36; 12.71) p < .0001 and granulomatous-lymphocytic interstitial lung disease: 4.85 (1.63; 14.39) p = 0.005. Diagnostic delay (median: 4 years) was associated with a higher risk of death: 1.04 (1.02; 1.06) p = .0003, bronchiectasis: 1.03 (1.01; 1.04) p = .0001, solid tumor: 1.08 (1.04; 1.11) p < .0001 and enteropathy: 1.02 (1.00; 1.05) p = .0447 and stayed unchanged over four decades (p = .228).
Conclusions: While the societal burden of CVID may seem moderate, it is severe to the individual patient. Delay in CVID diagnosis may constitute a modifiable risk factor of serious comorbidities and death but showed no improvement. Tools supporting timely CVID diagnosis should be developed with high priority.
Keywords: Burden of disease; Common variable immunodeficiency; DALY; Diagnostic delay; Health economics; Primary antibody deficiency; Primary immunodeficiency.
Conflict of interest statement
Ethics approval and consent to participate
All included patients signed a consent form for collection and use of their personal data for research purposes:
Consent for publication
All included patients signed a consent form giving their permission for the publication of the research results based on the analysis of the collected anonymised data:
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Orange JS, Glessner JT, Resnick E, Sullivan KE, Lucas M, Ferry B, Kim CE, Hou C, Wang F, Chiavacci R, Kugathasan S, Sleasman JW, Baldassano R, Perez EE, Chapel H, Cunningham-Rundles C, Hakonarson H. Genome-wide association identifies diverse causes of common variable immunodeficiency. J Allergy Clin Immunol. 2011;127(6):1360–7.e6. doi: 10.1016/j.jaci.2011.02.039. - DOI - PMC - PubMed
-
- Bonilla FA, Barlan I, Chapel H, Costa-Carvalho BT, Cunningham-Rundles C, de la Morena MT, Espinosa-Rosales FJ, Hammarström L, Nonoyama S, Quinti I, Routes JM, Tang ML, Warnatz K. International Consensus Document (ICON): Common Variable Immunodeficiency Disorders. J Allergy Clin Immunol Pract. 2016;4(1):38–59. doi: 10.1016/j.jaip.2015.07.025. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
