

SCOT: a comparison of cost-effectiveness from a large randomised phase III trial of two durations of adjuvant Oxaliplatin combination chemotherapy for colorectal cancer
- PMID: 30420616
- PMCID: PMC6265336
- DOI: 10.1038/s41416-018-0319-z
SCOT: a comparison of cost-effectiveness from a large randomised phase III trial of two durations of adjuvant Oxaliplatin combination chemotherapy for colorectal cancer
Abstract
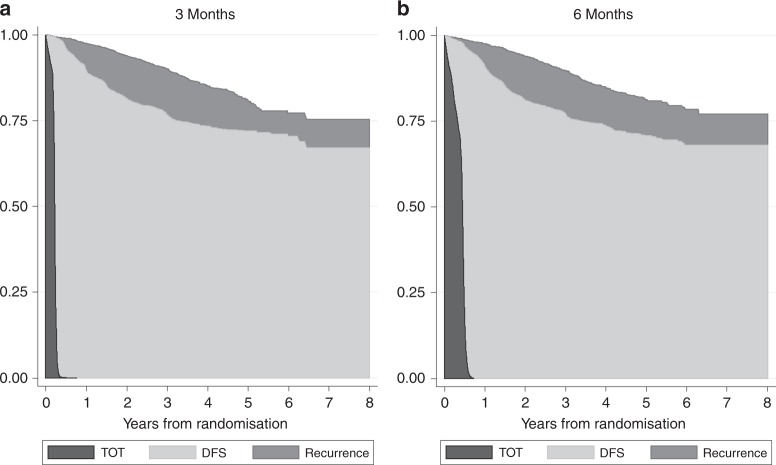
Background: The Short Course Oncology Therapy (SCOT) study is an international, multicentre, non-inferiority randomised controlled trial assessing the efficacy, toxicity, and cost-effectiveness of 3 months (3 M) versus the usually given 6 months (6 M) of adjuvant chemotherapy in colorectal cancer.
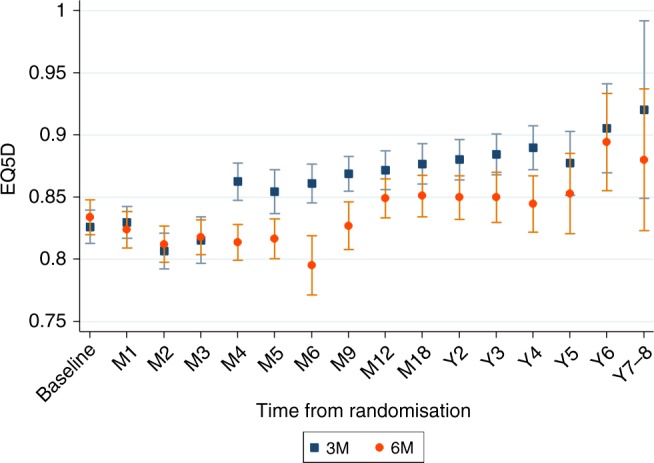
Methods: In total, 6088 patients with fully resected high-risk stage II or stage III colorectal cancer were randomised and followed up for 3-8 years. The within-trial cost-effectiveness analysis from a UK health-care perspective is presented using the resource use data, quality of life (EQ-5D-3L), time on treatment (ToT), disease-free survival after treatment (DFS) and overall survival (OS) data. Quality-adjusted partitioned survival analysis and Kaplan-Meier Sample Average Estimator estimated QALYs and costs. Probabilistic sensitivity and subgroup analysis was undertaken.
Results: The 3 M arm is less costly (-£4881; 95% CI: -£6269; -£3492) and entails (non-significant) QALY gains (0.08; 95% CI: -0.086; 0.230) due to a better significant quality of life. The net monetary benefit was significantly higher in 3 M under a wide range of monetary values of a QALY. The subgroup analysis found similar results for patients in the CAPOX regimen. However, for the FOLFOX regimen, 3 M had lower QALYs than 6 M (not statistically significant).
Conclusions: Overall, 3 M dominates 6 M with no significant detrimental impact on QALYs. The results provide the economic case that a 3 M treatment strategy should be considered a new standard of care.
Conflict of interest statement
T.I. reports Honoraria from Lilly Advisory Boards for Servier, Roche and Celgene Travel expenses from Bayer and Servier outside the submitted work. J.B. reports personal fees from Servier, Celgene and Merck, and non financial supports from Merck Sharpe and Dohme outside the submitted work. C.W. reports grants from sirtex-european symposium Nov 2016, outside the submitted work. D.C. reports grants from Amgen, AstraZeneca, Bayer, Celgene, Merrimack, MedImmune, Merck Serono and Sanofi, outside the submitted work. J.C. reports grants from MRC and CRUK, and confirms that he is currently an employee with Celgene Corporation. K.A.B. reports grants from Medical Research Council during the conduct of the study. J.T. reports other from Amgen, Bayer, Boehringer Ingelheim, Celgene, Chugai, Lilly, MSD, Merck Serono, Novartis, Pfizer, Roche, Sanofi, Symphogen, Taiho and Takeda, outside the submitted work. A.W. is involved in research that is funded by drug companies that provide the drugs for the study. She has been co-investigator in trials funded by Roche that provide Capecitabine used in this study. B.G. sits on the Advisory Board for PledPharma AB.
Figures
References
-
- CRUK. Bowel cancer statistics 2016 [http://www.cancerresearchuk.org/health-professional/cancer-statistics/st....
-
- Haller D., Catalano P., Macdonald J., Mayer R., editors. Fluorouracil (FU), leucovorin (LV) and levamisole (LEV) adjuvant therapy for colon cancer: five-year final report of INT-0089. Proc Am Soc Clin Oncol; 1998.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
