

Fecal microbiota transplantation for refractory immune checkpoint inhibitor-associated colitis
- PMID: 30420754
- PMCID: PMC6322556
- DOI: 10.1038/s41591-018-0238-9
Fecal microbiota transplantation for refractory immune checkpoint inhibitor-associated colitis
Erratum in
-
Author Correction: Fecal microbiota transplantation for refractory immune checkpoint inhibitor-associated colitis.Nat Med. 2019 Jan;25(1):188. doi: 10.1038/s41591-018-0305-2. Nat Med. 2019. PMID: 30479380
Abstract
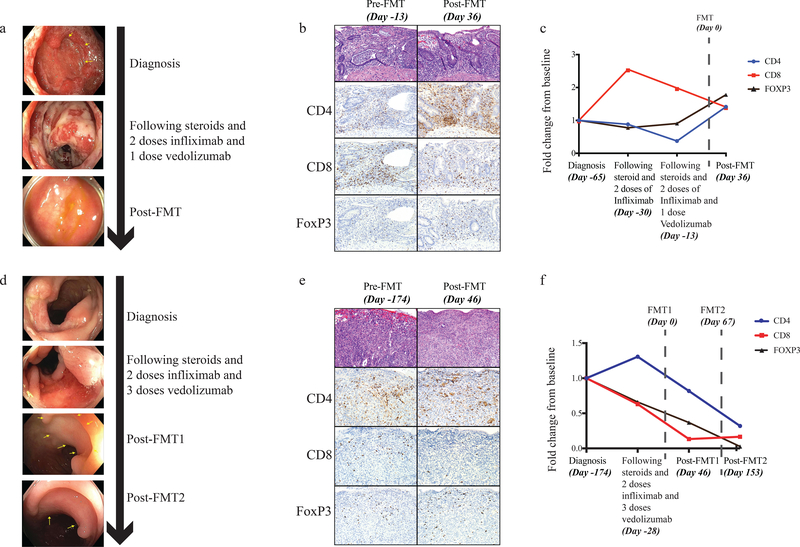
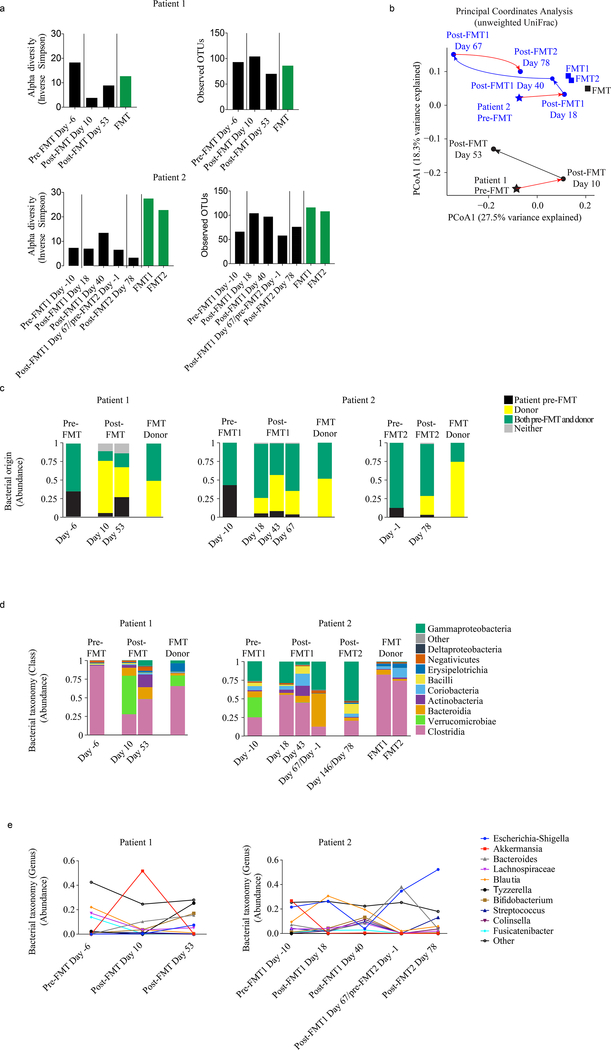
We report the first case series of immune checkpoint inhibitors (ICI)-associated colitis successfully treated with fecal microbiota transplantation, with reconstitution of the gut microbiome and a relative increase in the proportion of regulatory T-cells within the colonic mucosa. These preliminary data provide evidence that modulation of the gut microbiome may abrogate ICI-associated colitis.
Conflict of interest statement
Competing Interests Declaration:
J.A.W and V.G. are inventors on a US patent application (PCT/US17/53,717) submitted by The University of Texas MD Anderson Cancer Center that covers methods to enhance checkpoint blockade therapy by the microbiome. J.A.W. is a clinical and scientific advisor at Microbiome DX and a consultant at Biothera Pharma, Merck Sharp, and Dohme. J.A.W. has honoraria from speakers’ bureau of Dava Oncology, Bristol-Myers Squibb, Gilead, Illumina, Omniprex, Imedex and is an advisory board member for GlaxoSmithKline, Novartis, and Roche/Genentech, Astra-Zeneca. V.G. is a consultant at Microbiome DX, and reports honoraria from ExpertConnect. R.R.J. is on the scientific advisory board for Seres Therapeutics, Inc., has consulted for Ziopharm Oncology and Microbiome Dx, and holds patents licensed to Seres Therapeutics, Inc. M.T.T. serves on the advisory board for Novartis, Seattle Genetics and Myriad Genetics. J.A.W., P.S., and J.P.A. are members of the Parker Institute for Cancer Immunotherapy at MD Anderson Cancer Center. P.S. is a consultant for Bristol-Myers Squibb, Jounce Therapeutics, Helsinn, and GlaxoSmithKline and is also a stockholder from Jounce Therapeutics. J.P.A. is a consultant and stockholder for Jounce Therapeutics, receives royalties from Bristol-Myers Squibb, and has intellectual property with Bristol-Myers Squibb and Merck. The other authors declare no competing interests.
Figures
Comment in
-
FMT for drug-induced colitis.Nat Rev Gastroenterol Hepatol. 2019 Jan;16(1):4. doi: 10.1038/s41575-018-0092-8. Nat Rev Gastroenterol Hepatol. 2019. PMID: 30510291 No abstract available.
-
One man's trash-another man's treasure: fecal transplantation.Hepatobiliary Surg Nutr. 2019 Dec;8(6):623-625. doi: 10.21037/hbsn.2019.06.05. Hepatobiliary Surg Nutr. 2019. PMID: 31929989 Free PMC article. No abstract available.
References
-
- Michot JM, et al. Immune-related adverse events with immune checkpoint blockade: a comprehensive review. Eur J Cancer 54, 139–148 (2016). - PubMed
-
- Cramer P & Bresalier RS Gastrointestinal and Hepatic Complications of Immune Checkpoint Inhibitors. Curr Gastroenterol Rep 19, 3 (2017). - PubMed
-
- Chen JH, Pezhouh MK, Lauwers GY & Masia R Histopathologic Features of Colitis Due to Immunotherapy With Anti-PD-1 Antibodies. Am J Surg Pathol 41, 643–654 (2017). - PubMed
-
- Dadu R, Zobniw C & Diab A Managing Adverse Events With Immune Checkpoint Agents. Cancer J 22, 121–129 (2016). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
